

Medetomidine is a veterinary sedative now appearing in street fentanyl across the United States, causing prolonged overdoses and severe withdrawal.
Originally developed for animal anesthesia, this alpha-2 adrenergic agonist has become a dangerous adulterant that complicates overdose response and introduces a life-threatening withdrawal syndrome marked by extreme blood pressure spikes, vomiting, and delirium.
This article explains what medetomidine is, how it works, and why its spread in the illegal drug supply has become a national emergency requiring new clinical protocols and faster public health response.
What is Medetomidine?
Medetomidine is an alpha-2 adrenergic agonist sedative used in veterinary medicine to sedate and provide pain relief in dogs and cats. It is not approved for human use in the United States.
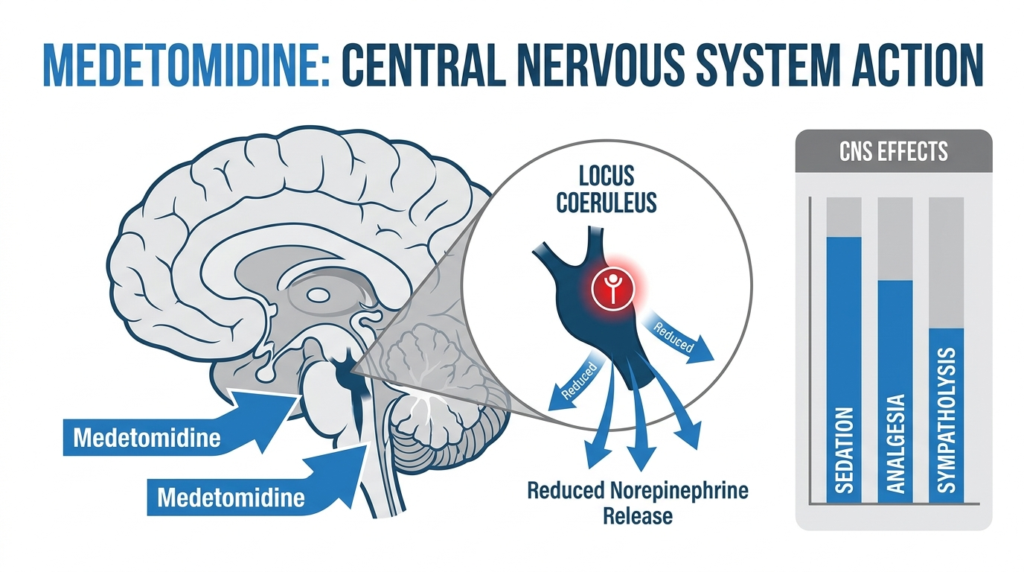
The drug works by activating alpha-2 receptors in the brain and spinal cord, reducing norepinephrine release and suppressing sympathetic nervous system activity. This produces dose-dependent sedation ranging from moderate to deep, along with analgesia and muscle relaxation.
Veterinarians use medetomidine for restraint, premedication before surgery, and as part of combination anesthetic protocols. It is marketed as a racemic mixture containing two mirror-image molecules: dexmedetomidine and levomedetomidine.
Dexmedetomidine is the active component and is separately approved for human hospital sedation, but racemic medetomidine itself has no legitimate human medical application.
The drug’s potency is significant. Medetomidine is described by the CDC as more potent and longer-acting than both xylazine and clonidine, two related alpha-2 agonists.
This higher potency explains why medetomidine produces more profound sedation and more severe withdrawal symptoms when exposure stops abruptly.
What is Medetomidine Used For in Veterinary Medicine?
In dogs, medetomidine produces reliable sedation and analgesia across a range of procedures. Veterinarians administer it for handling and restraint, as a premedication before general anesthesia, and in combination with other drugs to reduce the doses of more dangerous anesthetics.
The NOAH Compendium notes that medetomidine has a marked anesthetic-sparing effect, meaning it significantly reduces the amount of agents like thiopentone, halothane, and propofol needed during surgery.
In cats, approved uses include sedation for restraint, combination with ketamine for anesthesia induction, pairing with butorphanol for sedation and pain relief, and use as a premedication before other anesthetic agents. The sedation level in cats is also dose-dependent and can range from moderate to deep.
This veterinary utility is based on predictable pharmacology: medetomidine suppresses arousal and sympathetic tone in a controlled clinical setting. The same properties that make it useful in animal care become dangerous when people unknowingly consume it mixed with fentanyl.
How Medetomidine Works?
Medetomidine acts primarily as an alpha-2 adrenergic receptor agonist in the central nervous system. By activating these receptors in the brain and spinal cord, it decreases noradrenergic activity and reduces sympathetic outflow. This mechanism produces several effects:
Central nervous system effects include sedation through decreased activity in the locus coeruleus, a brain region involved in wakefulness and arousal. The drug also provides analgesia through both central and peripheral mechanisms.
These effects explain why intoxicated patients remain deeply sedated even after naloxone restores breathing from co-occurring opioid toxicity. Naloxone reverses opioid receptor-mediated respiratory depression but does not reverse medetomidine’s alpha-2 agonist suppression of arousal.
Cardiovascular effects arise from both central and peripheral alpha-2 agonism. Public health reports describe medetomidine intoxication as producing marked bradycardia, hypotension, and sometimes initial hypertension before later blood pressure drops.
These hemodynamic changes distinguish medetomidine-containing intoxication from straightforward opioid overdose, which typically does not produce the same degree of sustained slow heart rate.
Withdrawal effects represent the opposite pattern. When regular medetomidine exposure stops abruptly, the body experiences sympathetic and autonomic rebound. This produces tachycardia, severe hypertension, tremor, anxiety, and other signs of autonomic hyperactivity.
Understanding this bidirectional effect is essential for recognizing both intoxication and withdrawal.
Medetomidine Effects and Side Effects
Expected Effects in Veterinary Use
When used appropriately in animals, medetomidine’s desired effects include sedation, analgesia, muscle relaxation, facilitation of handling or restraint, premedication before anesthesia, and reduced dose requirements for other anesthetics. These effects are predictable and manageable in controlled veterinary settings.
Adverse Effects and Toxicity
Across veterinary and toxicology sources, medetomidine’s adverse effect profile includes bradycardia, hypotension, profound sedation, central nervous system depression, hyperglycemia, hallucinations, and possible biphasic blood pressure changes.
The key concern is not that medetomidine has unusual toxicity for an alpha-2 agonist, but that the same expected pharmacology becomes dangerous and difficult to manage when exposure is unplanned, mixed with opioids, and not easily detectable on standard hospital toxicology screens.
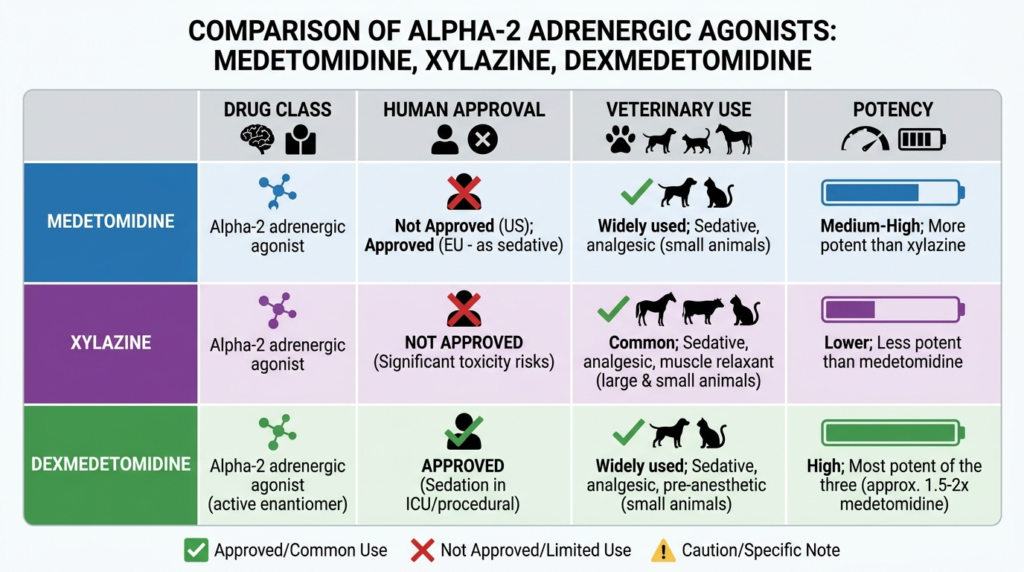
Comparison With Xylazine and Dexmedetomidine
Medetomidine is often compared with xylazine because both are veterinary alpha-2 agonists now found in the illegal drug supply. It is also compared with dexmedetomidine because dexmedetomidine is its active enantiomer and an established human sedative.
| Feature | Medetomidine | Xylazine | Dexmedetomidine |
|---|---|---|---|
| Drug class | Alpha-2 agonist | Alpha-2 agonist | Alpha-2 agonist |
| Human approval | No | No | Yes |
| Veterinary use | Yes | Yes | Limited |
| Relative potency | More potent than xylazine | Less potent | Active enantiomer |
| Illicit supply role | Increasing adulterant | Established adulterant | Not typically illicit |
| Intoxication signs | Profound sedation, bradycardia | Sedation, bradycardia | Sedation, bradycardia |
| Withdrawal concern | Severe, ICU-level | Recognized | Known in hospital settings |
Sources indicate medetomidine is more potent and longer-lasting than xylazine, which may explain why intoxication and withdrawal can be more severe and prolonged.
Some expert summaries estimate medetomidine may be 100 to 200 times more potent than xylazine, though these claims should be treated cautiously as they come from local health summaries rather than national consensus guidance.
Medetomidine Overdose: Recognition and Response
Clinical Presentation of Intoxication
Human intoxication from medetomidine in the illicit opioid supply is now characterized with increasing clarity.
The CDC states that medetomidine can cause profound sedation, marked bradycardia, and hypotension. The Chicago MMWR report found that patients with confirmed cases commonly had bradycardia and no or only partial response to naloxone.
Typical findings across official and peer-reviewed sources include depressed mental status or prolonged unresponsiveness, pinpoint pupils when opioids are co-involved, hypoxemia or respiratory compromise from opioid co-exposure, sinus bradycardia often striking enough to stand out, low blood pressure with some hypertensive episodes, and prolonged sedation after naloxone has improved ventilation.
Why Naloxone May Seem Ineffective
A major clinical problem is that medetomidine exposure can make naloxone appear ineffective even when it is successfully treating the opioid component of overdose.
The CDC repeatedly emphasizes that naloxone does not reverse medetomidine itself, but naloxone should still be given because fentanyl is involved in most medetomidine-related overdoses. The goal is to restore breathing, not necessarily full alertness.
The MMWR Chicago investigation reinforces this by showing that fentanyl was identified in all drug samples and blood specimens containing medetomidine.
Thus, continued heavy sedation after naloxone does not mean naloxone was pointless. It means clinicians and responders may be dealing with a mixed opioid plus alpha-2 agonist intoxication.
Community Response Recommendations
The CDC’s practical recommendation is to repeat naloxone every two to three minutes as needed to achieve adequate ventilation, place the person in the recovery position, and recognize that medetomidine-related sedation will wear off over time.
Call 911 and provide ongoing monitoring. This guidance resolves a common confusion: if the person remains sedated after naloxone, bystanders may mistakenly think more and more naloxone is required purely to achieve consciousness. The CDC instead emphasizes breathing as the critical endpoint.
Clinical Management
For clinicians, current official recommendations include considering medetomidine when there is prolonged sedation after suspected opioid overdose despite naloxone, providing supportive cardiorespiratory care, watching for bradycardia and hypotension, considering comprehensive drug screening including blood testing for medetomidine when available, and consulting a toxicologist or poison center. In the Chicago cluster, some patients required atropine for bradycardia.
Medetomidine Withdrawal Symptoms
The most distinctive and clinically disruptive feature of medetomidine may not be intoxication but withdrawal.
The CDC states that stopping medetomidine after regular use can precipitate severe withdrawal resembling clonidine withdrawal, with symptoms including tachycardia, severe hypertension, anxiety, tremor, fluctuating alertness, chest pain, and intractable nausea and vomiting.
Core Symptom Cluster
Across Philadelphia, Pittsburgh, CDC guidance, and city-level advisories, the symptom pattern is remarkably consistent. The most characteristic symptoms and signs include:
- Tachycardia
- Severe hypertension
- Agitation and anxiety
- Tremor, often without clonus or hyperreflexia
- Nausea and vomiting, frequently severe or intractable
- Fluctuating alertness, delirium, or encephalopathy in severe cases
- Diaphoresis
- Restlessness
- Chest pain in some severe cases
In Philadelphia, the MMWR field report identified 165 patients with one or more of these symptoms resistant to escalating conventional treatment: agitation, anxiety, severe hypertension, tachycardia, tremor without clonus or hyperreflexivity, and vomiting.
Timing of Symptom Onset
The syndrome often begins quickly. The CDC states symptoms may begin within hours of last use and peak 18 to 36 hours later. Other clinical syntheses describe onset within six to 24 hours of the last use.
A particularly important operational point from the Pittsburgh report is that many patients did not arrive at the emergency department already in full withdrawal. Eight of ten confirmed cases developed symptoms several hours after arrival, suggesting that patients may appear stable or only mildly symptomatic initially and then abruptly deteriorate.
Distinguishing Features From Opioid Withdrawal
Standard opioid withdrawal is typically uncomfortable and distressing, but it is not usually characterized by severe hypertension, marked tachycardia beyond routine withdrawal, fluctuating alertness or delirium, refractory vomiting with autonomic storm, ICU-level hemodynamic management, or need for dexmedetomidine infusion. Yet these are exactly the features repeatedly documented in medetomidine withdrawal.
Philadelphia clinicians specifically reported that symptoms did not resolve with medications that had previously been effective for fentanyl and xylazine withdrawal.
Local public health summaries similarly found that emergency department withdrawal protocols became less effective after medetomidine entered the supply; patients had smaller reductions in Clinical Opioid Withdrawal Scale scores, higher ICU admission rates, and more patient-directed discharges.
Medetomidine Withdrawal Treatment
Core Treatment Principle
The most consistent treatment principle across public health advisories, MMWR reports, and hospital guidance is that care must address both the patient’s concurrent opioid withdrawal or opioid use disorder and the medetomidine-related autonomic rebound.
This dual-treatment model is central because patients are usually exposed to fentanyl plus medetomidine, not medetomidine alone.
Clonidine
Clonidine is the most consistently recommended oral alpha-2 agonist option for suspected medetomidine withdrawal when the patient can tolerate oral therapy and is hemodynamically suitable.
It directly addresses autonomic hyperactivity and pharmacologically resembles the alpha-2 agonist effect being withdrawn. Regional protocols emphasize early initiation of clonidine rather than waiting for severe escalation.
Clonidine serves as initial therapy in mild-to-moderate suspected withdrawal, a bridge or adjunct while opioid therapy is initiated, and step-down therapy after ICU dexmedetomidine infusion. Some protocols combine oral clonidine with transdermal clonidine patch, guanfacine, and occasionally tizanidine in refractory cases.
Dexmedetomidine Infusion
Dexmedetomidine is the best-supported hospital therapy for severe medetomidine withdrawal. In Philadelphia, 137 of 165 patients were treated with and responded to dexmedetomidine infusion.
In Pittsburgh, nine of ten confirmed cases admitted to ICU received dexmedetomidine for autonomic hyperactivity. The CDC explicitly notes that the syndrome in Philadelphia was resistant to prior regimens but responsive to dexmedetomidine.
Dexmedetomidine works because it is an enantiomerically related alpha-2 agonist and therefore directly treats the withdrawal mechanism more effectively than opioid medications or nonspecific sedatives.
It is generally indicated when there is severe hypertension or tachycardia, uncontrolled vomiting, encephalopathy or delirium, failure of oral clonidine-based therapy, inability to tolerate oral medications, or ICU-level instability.
Methadone or Buprenorphine
Even though opioid medications do not fully treat medetomidine withdrawal, they remain necessary because most affected patients also have opioid dependence and concurrent fentanyl withdrawal.
The key principle is to treat opioid withdrawal and medetomidine withdrawal simultaneously, not sequentially. Hospital protocols recommend either methadone initiation or buprenorphine induction or micro-induction while alpha-2 agonist therapy is being administered.
Antiemetics and Symptom-Directed Care
Nausea and vomiting are often severe and require active treatment. Several guidance documents note that ondansetron may be ineffective.
Alternative choices frequently recommended include prochlorperazine, droperidol, metoclopramide, and olanzapine in some protocols.
When to Escalate to ICU Care
The Philadelphia data showing 91 percent ICU admission are not incidental. ICU-level care is often required because patients may need continuous hemodynamic monitoring, dexmedetomidine infusion, airway protection, management of encephalopathy, and rapid titration of sedatives and antihypertensive effect via withdrawal control.
Escalation is especially warranted when there is severe or rapidly rising blood pressure, persistent tachycardia, fluctuating alertness, uncontrolled vomiting, chest pain, or refractory symptoms despite oral treatment.
Emergence in the Illegal Drug Supply
Timeline and Geographic Spread
Medetomidine was first identified in the illegal drug supply in 2021. From mid-2023 to mid-2024, it appeared sporadically in multiple jurisdictions including Chicago, Philadelphia, and Pittsburgh. By late July 2024, it had been detected in drug samples and biologic specimens in at least 18 states and the District of Columbia.
The scale of expansion after that point was substantial. NFLIS reports rose from 247 in 2023 to 2,616 in 2024, a 950 percent increase. Reports continued rising sharply to 8,233 in 2025. These figures indicate a rapidly diffusing adulterant rather than a localized anomaly.
Philadelphia as the Leading Indicator
Philadelphia offers the clearest example of how fast medetomidine can transform a regional drug market. During the last four months of 2024, medetomidine was detected in 72 percent of illegal opioid samples tested, while xylazine detection dropped from 98 percent to 31 percent.
Additional local public health reporting showed that from May 2024 to November 2024, medetomidine-positive dope samples rose from 29 percent to 87 percent, while xylazine-positive samples fell from 97 percent to 42 percent.
A later public-facing summary reported that medetomidine was detected in about 15 percent of all fatal overdoses in Philadelphia between May 2024 and May 2025, further reinforcing its public health significance.
Evidence of Clandestine Synthesis
The CDC’s 2026 Health Advisory makes a particularly important analytical point: illicit samples showed racemic medetomidine without preservatives typical of medical or veterinary products, making diversion of pharmaceutical-grade material unlikely and suggesting clandestine manufacture.
This matters because it changes how policymakers should think about control strategies. If the main source were veterinary diversion, interventions would focus more narrowly on veterinary supply chains. The evidence instead points toward broader illicit synthesis and trafficking.
Major Outbreaks and Epidemiologic Evidence
Chicago, May 2024
The Chicago cluster remains one of the most important published investigations because it provides robust clinical and epidemiologic detail.
CDC investigators identified during May 11 to 17, 2024, twelve confirmed cases, 26 probable cases, and 140 suspected cases involving medetomidine mixed with opioids, making it the largest reported cluster of confirmed medetomidine-involved overdoses.
Key findings included that the event was first recognized after hospitals and the Illinois Poison Center noticed atypical opioid-overdose presentations, especially on Chicago’s West Side. Fentanyl was present in all medetomidine-positive blood and drug samples.
Most confirmed patients had bradycardia, many showed no or only partial response to naloxone, and at least 16 people were hospitalized and one died.
Philadelphia Withdrawal Reports
If Chicago clarified intoxication, Philadelphia clarified withdrawal. The CDC’s 2026 HAN states that from September 2024 to January 2025, 165 patients across three Philadelphia health systems were hospitalized for fentanyl withdrawal complicated by severe autonomic dysfunction temporally associated with medetomidine in the supply. Among these patients, 150 required ICU care and 39 required intubation or mechanical ventilation.
These reports establish several advanced clinical lessons: withdrawal can be more distinctive than intoxication, routine screens may miss medetomidine exposure, severe cases often require ICU-level management, and the burden on emergency and inpatient systems can be substantial.
Diagnostic Challenges
Medetomidine withdrawal is often diagnosed clinically rather than through immediate laboratory confirmation. Several factors complicate diagnosis: the patient may not know medetomidine was present, routine toxicology may confirm fentanyl but miss medetomidine, symptoms overlap partially with opioid or xylazine withdrawal, and deterioration may occur hours after presentation.
One of the deepest and most important research insights comes from the Pittsburgh analysis: medetomidine parent compound was detected in only two patients on comprehensive urine screening, but retrospective metabolite analysis identified medetomidine exposure in all ten tested samples. This finding leads to a clinically decisive rule: a negative medetomidine screen does not rule out medetomidine exposure or withdrawal.
Clinicians should strongly suspect medetomidine withdrawal when a patient with fentanyl or street opioid exposure has severe tachycardia, severe hypertension, tremor without clonus or hyperreflexia, severe nausea or vomiting, waxing and waning alertness or delirium, and poor response to escalating opioid withdrawal treatment.
Complications and Risks
Medetomidine withdrawal is dangerous because it is not merely uncomfortable. It can produce serious end-organ complications. Severe sympathetic rebound can lead to myocardial injury, non-ST elevation myocardial infarction in reported cases, and cardiomyopathy in some institutional guidance. The broader Philadelphia multicenter study found myocardial injury in 29 percent of patients.
Reported neurologic complications include encephalopathy, posterior reversible encephalopathy syndrome, fluctuating alertness or delirium, and less commonly seizure-like activity or true seizures often with co-exposures. Encephalopathy occurred in 35 percent of patients in the larger Philadelphia cohort.
Institutional guidance and expert summaries note metabolic and systemic complications including hypokalemia, lactic acidosis, QTc prolongation, and severe dehydration risk from vomiting. The syndrome also carries system-level risks including high ICU occupancy, intubation and sedation needs, prolonged ED observation, heavy toxicology consultation demand, and high rates of patient-directed discharge.
Public Health Implications
Medetomidine matters not only because it increases overdose complexity, but because it changes the structure of harm in the illicit opioid market.
It adds a second dangerous sedative layer to fentanyl, creating a compound toxidrome of opioid respiratory depression plus alpha-2 agonist sedation and cardiovascular suppression. It complicates community overdose response because when breathing improves but consciousness does not, bystanders may become confused about whether naloxone worked.
It creates a distinct withdrawal burden. Unlike xylazine’s already serious harms, medetomidine appears to introduce a particularly severe autonomic withdrawal syndrome, straining ED and ICU resources. Philadelphia’s experience suggests the resulting health-system burden can be very large in a short time.
The growth trajectory, geographic spread, and evidence of clandestine synthesis all suggest medetomidine’s rise is a market-level phenomenon. It is reasonable to infer that medetomidine is being added because it changes the perceived or functional profile of illicit opioids, potentially prolonging sedative effects or modifying subjective effects.
The Chicago investigation showed that rapid recognition depended on hospitals, poison centers, toxicology laboratories, emergency services, and public health agencies working together. Medetomidine is therefore a model case for why emerging-adulterant response cannot rely on a single surveillance stream.
Conclusion
Based on the strongest and most current evidence, medetomidine should be regarded not merely as another fentanyl adulterant, but as a clinically transformative one. It changes overdose presentation, prolongs sedation after opioid reversal, and introduces a severe withdrawal syndrome that is distinct enough to alter triage, inpatient care, and public health surveillance.
Among emerging adulterants, its practical danger lies less in mysterious novelty than in the fact that it reliably adds a second pharmacologic crisis on top of fentanyl: first a mixed opioid–alpha-2 intoxication, then in regular users a potentially violent autonomic withdrawal syndrome.
Its spread is rapid and national, not isolated. Its co-occurrence with fentanyl is extremely common in documented cases. Its physiologic signature is recognizable and clinically important. Its withdrawal burden may be more system-straining than its intoxication burden. Current detection and treatment infrastructure is not yet fully adapted to it.
If the question is what medetomidine is and what it is used for, the complete answer is that it is a veterinary alpha-2 adrenergic agonist sedative and analgesic used in dogs and cats for sedation, restraint, premedication, and anesthesia support. It works by reducing central norepinephrine release and sympathetic activity. Its predictable effects include sedation, analgesia, bradycardia, and hypotension.
In the illicit drug supply, especially when mixed with fentanyl, it can cause profound prolonged sedation, marked bradycardia, incomplete apparent response to naloxone, and severe withdrawal with hypertension, tachycardia, vomiting, tremor, and fluctuating alertness.
Naloxone still should be used in suspected overdoses because fentanyl is usually co-involved, but response should be judged by breathing, not wakefulness. The strongest current public health evidence indicates medetomidine is an expanding national overdose and withdrawal threat that requires clinical vigilance, better testing, and coordinated surveillance.
If you or someone you know is struggling with substance use or experiencing withdrawal symptoms, we’re here to help you. Reach out to Thoroughbred Wellness and Recovery today and meet our addiction counseling professionals who understand the complexities of today’s drug supply and can provide comprehensive and compassionate care.








