

Carfentanil is an ultra‑potent synthetic opioid that can cause fatal overdose at microgram doses, often hidden in fentanyl products without the user’s knowledge.
Recent CDC surveillance shows a sevenfold increase in carfentanil‑involved overdose deaths between early 2023 and early 2024, with detections now reported across 37 states.
This article explains how to recognize carfentanil overdose symptoms, understand its effects and risks, identify signs of abuse or dependence, and respond effectively to save lives.
What is Carfentanil?
Carfentanil is a fentanyl analog with no approved medical use in humans. Originally developed for veterinary use in large animals, it is approximately 100 times more potent than fentanyl and 10,000 times more potent than morphine.
Unlike prescription opioids or even illicit fentanyl, carfentanil was never intended for human consumption and carries extreme overdose risk at extraordinarily small quantities.
The drug acts as a powerful agonist at the μ‑opioid receptor, producing intense respiratory depression, sedation, and loss of consciousness. Because only tiny amounts are needed to alter potency, carfentanil is often mixed into other products without users recognizing it.
This hidden contamination is what makes carfentanil one of the most dangerous substances in the current U.S. overdose crisis.
The Current Carfentanil Threat in the United States
The most important recent evidence comes from the CDC’s December 2024 analysis of overdose death data.
Researchers found that overdose deaths with carfentanil detected increased about sevenfold, from 29 in January through June 2023 to 238 in January through June 2024. During that period, carfentanil was detected in overdose deaths in 37 states, with the highest burden east of the Mississippi River.
Critically, approximately 87% of deaths with carfentanil detected also had illegally manufactured fentanyl present. This means carfentanil is now primarily a hidden adulterant in fentanyl products rather than a distinct drug people intentionally seek.
The contemporary concern is less about people choosing carfentanil and more about unknowing exposure through contaminated fentanyl, heroin, counterfeit pills, or even cocaine and methamphetamine.
How Carfentanil Enters the Drug Supply?
Carfentanil most often appears as a hidden contaminant or adulterant. The strongest evidence points to three main pathways:
- Mixed into fentanyl products: The high rate of co‑detection with illegally manufactured fentanyl strongly suggests carfentanil is being mixed into fentanyl powders, pills, and other formulations.
- Contamination of other street drugs: Earlier synthetic opioid literature notes that fentanyl analogs may be found with heroin, cocaine, and methamphetamine, increasing risk for people not intentionally using opioids.
- Counterfeit tablets and powders: Recent laboratory alerts describe carfentanil appearing in counterfeit tablets and powders, underscoring its role in unpredictable illicit formulations.
A crucial practical issue is that standard fentanyl test strips may not reliably detect carfentanil. Even if a fentanyl test strip result is negative, users should remain cautious because test strips might not detect more potent fentanyl‑like drugs such as carfentanil.
This means people often cannot identify carfentanil exposure before toxicity occurs.
Carfentanil Effects: What Happens in the Body?
Like fentanyl and related opioids, carfentanil exerts its effects primarily through μ‑opioid receptor activation. This produces several effects:
- Analgesia: Extreme pain relief, though this is irrelevant in illicit exposure contexts
- Euphoria: Intense but brief high that may drive repeated use
- Sedation: Profound drowsiness and loss of consciousness
- Respiratory depression: Slowed or stopped breathing, the primary cause of death
- Miosis: Pinpoint pupils
- Bradycardia: Slowed heart rate
- Hypotension: Dangerously low blood pressure
The specific reason overdose is so dangerous is that opioid toxicity suppresses the brainstem drive to breathe.
Carfentanil’s extreme potency means this respiratory depression can occur rapidly and profoundly, even at blood concentrations that appear very low analytically.
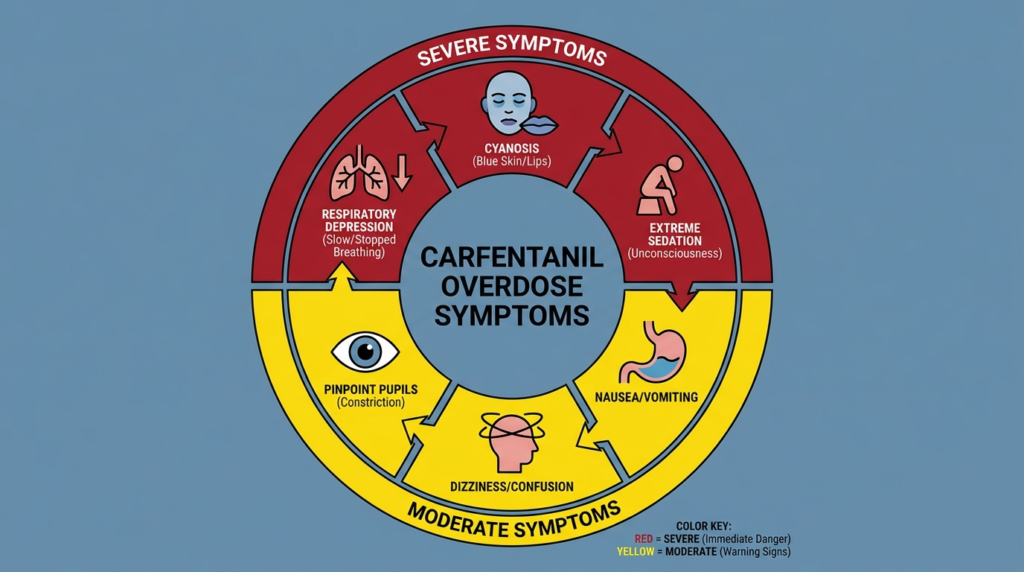
Carfentanil Overdose Symptoms: Recognizing a Life‑Threatening Emergency
The most reliable practical rule is this: assume any severe opioid overdose could involve carfentanil if the person is unresponsive, breathing slowly or not at all, turning blue, and naloxone response is incomplete or requires repeated doses.
Core Overdose Signs
A review of reported carfentanil toxicity identified the following presentations:
- Rapid loss of consciousness
- Respiratory depression or stopped breathing
- Cyanosis (blue or purple lips, fingernails, or skin)
- Pinpoint pupils
- Disorientation or confusion before collapse
- Vomiting
- Bradycardia (slow heart rate)
- Hypotension (low blood pressure)
- Gurgling, snoring, choking, or agonal breathing
- Limp body
- Pale or clammy skin
- Lack of response to verbal or physical stimuli
A confirmed recreational carfentanil exposure case described a patient who was hypotensive, tachycardic, hypopneic, cyanotic, with oxygen saturation of 70%, and unconscious until revived by intravenous naloxone.
Immediate Recognition Checklist
Red‑flag signs that require instant overdose response include:
- Person cannot be awakened
- Slow, shallow, irregular, or absent breathing
- Blue or purple lips or fingernails
- Pinpoint pupils
- Gurgling, snoring, choking, or agonal breathing
- Limp body
- Pale or clammy skin
- Slow heartbeat or no detectable pulse
- Severe confusion followed by collapse
- Vomiting with depressed consciousness
These signs are consistent with CDC and SAMHSA overdose recognition guidance for opioid poisoning generally, which remains appropriate for carfentanil because it is still an opioid overdose syndrome.
What Makes Carfentanil Overdose Different?
While carfentanil overdose shares the core opioid toxidrome with fentanyl and heroin, several features make it especially dangerous in practice:
Severe Toxicity at Low Concentrations
One of the most concerning insights from toxicological case reviews is that carfentanil can produce profound impairment at very low blood concentrations. This means that neither users nor responders should assume that a “small amount” exposure would produce only mild toxicity.
Faster Collapse is Plausible
The literature suggests that carfentanil overdoses may progress rapidly, though exact timing is difficult to generalize because many cases involve mixed substances, uncertain dose, uncertain route, and delayed discovery. In practice, witnesses may simply encounter a person already unresponsive.
More Naloxone Often Needed
Although naloxone works on carfentanil, current evidence suggests that carfentanil overdoses may require more doses than typical fentanyl overdoses.
A 2024 review concluded that most fentanyl overdoses can be reversed with two standard doses of intranasal or intramuscular naloxone, while carfentanil overdoses may require three or more doses.
The same article recommends distributing at minimum four standard doses of intranasal or intramuscular naloxone to each person, effectively two two‑dose kits, so dosing can continue in the event of carfentanil exposure or recurrent symptoms.
Carfentanil Abuse Signs and Symptoms
There is much less high‑quality evidence on a unique clinical syndrome of carfentanil addiction specifically than on carfentanil overdose.
Most dependence and addiction patterns are best understood under the broader category of opioid use disorder involving fentanyl‑class exposure, sometimes accidental.
Important Conceptual Clarification
For many individuals, “carfentanil use” is not intentional. The strongest current epidemiologic evidence indicates covert exposure through contaminated products. Therefore:
- Overdose signs are often clearer than abuse‑specific signs
- Addiction signs are often signs of opioid use disorder generally, not uniquely carfentanil
- Some people become physiologically dependent through repeated exposure to fentanyl‑adulterated supply that may intermittently contain carfentanil
Reliable Abuse and Dependence Indicators
Because carfentanil is an opioid analog, the practical signs of chronic misuse or dependence are most validly drawn from established opioid use disorder patterns:
- Craving opioids
- Escalating dose or frequency of use
- Inability to reduce use despite harm
- Withdrawal symptoms between uses
- Sedation or nodding
- Impaired concentration
- Mood changes
- Social withdrawal
- Risky polysubstance use
- Recurrent near‑overdose or overdose episodes
Withdrawal and Dependence
Available materials consistently describe withdrawal symptoms that are essentially opioid withdrawal symptoms:
- Nausea or vomiting
- Diarrhea
- Muscle aches
- Sweating
- Anxiety
- Insomnia
- Runny nose
- Tearing
- Irritability
- Increased pulse
- Elevated blood pressure
These are best interpreted not as unique signatures of carfentanil, but as manifestations of opioid dependence after repeated exposure.
Does Naloxone Work on Carfentanil?
This is one of the most important and most misunderstood points. The evidence strongly supports the conclusion that naloxone can reverse carfentanil toxicity.
Naloxone is used for overdoses involving heroin, fentanyl, carfentanil, hydrocodone, oxycodone, and methadone. A confirmed recreational carfentanil exposure case showed return of consciousness after intravenous naloxone. Recent mechanistic work questions the notion that carfentanil is “naloxone resistant” as a categorical claim.
But More Naloxone May Be Required
Although naloxone works, current evidence also suggests that carfentanil overdoses may require more doses than typical fentanyl overdoses. Several explanations are suggested across the literature:
- Very high agonist potency
- Receptor binding dynamics and slower dissociation
- Large effective opioid burden
- Recurrent toxicity after temporary reversal
- Mixed exposure with other sedating substances
Important Nuance
The evidence does not support the simplistic idea that all fentanyl or illegally manufactured fentanyl overdoses require dramatically higher naloxone doses than heroin.
A 2020 study found no significant difference in median naloxone dose among opioid overdose patients with fentanyl‑only, fentanyl plus opiate, or opiate‑only urine findings.
The best interpretation is:
- Typical fentanyl overdoses often respond to standard naloxone dosing
- Carfentanil is a notable exception where additional doses are more likely to be needed
- Field responders and bystanders should prepare for repeat dosing without assuming naloxone is futile
What to Do If You Suspect Carfentanil Overdose?
The strongest practical recommendations come from CDC, SAMHSA, and recent naloxone reviews. The currently recommended response protocol is a five‑step process:
Step 1: Check for Signs of Opioid Overdose
- Try to wake the person by shouting their name and rubbing the sternum
- Look for slow, absent, or gurgling breathing
- Check for blue lips or fingernails
Step 2: Call 911 Immediately
Do this as soon as overdose is suspected, not after naloxone “fails.” Calling emergency medical services is critical because field naloxone may be insufficient to fully reverse the overdose.
Step 3: Administer Naloxone
- Give the first naloxone dose according to product instructions
- If no response in the recommended interval, give another dose
- Continue repeat dosing as needed
Step 4: Support Breathing
- Open the airway
- Give rescue breaths if trained and able
- If no breathing or only very weak breathing, respiratory support is critical
Step 5: Stay with the Person
- Monitor closely for recurrence of sedation or slowed breathing
- Place in recovery position if breathing returns but the person is not fully alert
- Be ready to give more naloxone
When to Escalate Concern
You should assume a particularly dangerous exposure, including possible carfentanil or polysubstance involvement, if:
- The person remains unresponsive after two naloxone doses
- Breathing does not improve
- Breathing improves only briefly then worsens again
- The person has profound cyanosis or no detectable vital signs
- There is evidence of mixed‑drug use
Why Calling 911 Matters Even After Naloxone Works?
A major theme across the evidence is that naloxone is lifesaving but temporary. Giving naloxone is unlikely to cause harm even if the cause of unconsciousness is uncertain, but it is not a substitute for emergency medical care.
Reasons EMS is Still Necessary
- Naloxone may wear off before the opioid effect ends
- Carfentanil may require repeat or escalating dosing
- Respiratory support may be needed
- Co‑intoxicants may be present
- Aspiration, pulmonary edema, cardiac arrest, or hypoxic brain injury may already be developing
- New adulterants such as medetomidine may complicate the picture
Naloxone is not a substitute for emergency medical care, and redosing may be required, especially with synthetic opioids such as fentanyl or carfentanil.
Complications and Co‑Exposure Risks
One of the strongest connections across research branches is between CDC surveillance and clinical uncertainty.
Since about 87% of carfentanil‑involved deaths show illegally manufactured fentanyl co‑detection, most real‑world carfentanil cases are not pharmacologically “pure.”
This has several consequences:
- Clinical presentation may reflect more than one opioid
- Naloxone response may be incomplete or temporary
- Scene interpretation becomes difficult
- Toxicology findings must be interpreted cautiously

Emerging Adulterants That Naloxone Will Not Reverse
The 2026 CDC Health Alert Network on medetomidine adds a critical modern complication. Medetomidine, an emerging sedative adulterant in the illegal fentanyl supply, can cause profound sedation, bradycardia, hypotension, and severe withdrawal syndrome after repeated exposure.
Because fentanyl is involved in most overdoses involving medetomidine, opioid overdose reversal medications such as naloxone should still be administered to restore breathing, but prolonged sedation unresponsive to naloxone should raise suspicion for non‑opioid co‑exposure.
This creates a practical diagnostic trap. If a person exposed to fentanyl‑adulterated drugs remains profoundly sedated after naloxone, responders might wrongly conclude that naloxone “doesn’t work on carfentanil.” In reality, several possibilities exist:
- Insufficient naloxone for a potent opioid burden
- Recurrent opioid toxicity
- Mixed opioid plus medetomidine exposure
- Mixed opioid plus xylazine or benzodiazepine exposure
- Severe hypoxic injury already in progress
Limitations of Drug Checking
CDC supports fentanyl test strips as an inexpensive way to detect fentanyl in drug products, but explicitly warns that even a negative test should not reassure users completely because test strips may not detect more potent fentanyl‑like drugs such as carfentanil.
Why Toxicological Certainty is Hard
Carfentanil poses detection difficulties because:
- Concentrations can be extremely low
- Products may contain multiple opioids and adulterants
- Timing of sample collection matters
- Rapid metabolism may complicate interpretation
- Some field tools are not designed to identify specific analogs
Drug checking is useful as one layer of harm reduction but is not sufficient to manage carfentanil risk. The more reliable protective measures remain:
- Never using alone
- Carrying naloxone
- Carrying multiple doses
- Calling 911 immediately for suspected overdose
- Using supervised consumption settings where available
Carfentanil vs. Fentanyl vs. Other Opioid Overdoses
Carfentanil overdose shares the core opioid toxidrome with fentanyl and heroin: respiratory depression, miosis or pinpoint pupils, sedation or coma, cyanosis, bradycardia or hypotension in severe cases, and response to naloxone.
Differences That Matter in Practice
| Feature | Typical heroin/opioid overdose | Many fentanyl overdoses | Suspected carfentanil overdose |
|---|---|---|---|
| Severity | Variable | Often severe | Often very severe |
| Onset | Can be rapid | Rapid | Potentially very rapid |
| Naloxone response | Usually standard dosing effective | Often 1–2 standard doses effective | May require 3+ doses |
| Hidden exposure | Sometimes known | Often hidden | Very often hidden |
| Test strip detectability | N/A | Often detectable via fentanyl strips | May be missed by standard fentanyl strips |
| Modern supply role | Less dominant | Dominant illegally manufactured fentanyl supply | Potent adulterant layered into illegally manufactured fentanyl supply |
Why the “100 Times Stronger” Statement is Not Enough?
Stating that carfentanil is 100 times more potent than fentanyl is factually useful but operationally incomplete.
Potency does not map linearly onto field lethality because actual overdose risk depends on concentration in the product, route of administration, user tolerance, total dose consumed, presence of benzodiazepines, xylazine, medetomidine, alcohol, or other depressants, and speed of intervention.
The practical response must therefore be based on observed toxicity, not abstract potency.
Public Health Implications and Prevention
The most significant synthesis across surveillance and overdose‑response literature is that the major danger of carfentanil in 2026 is not merely that it exists, but that it exists inside a fentanyl‑saturated, unpredictable, polysubstance supply. This makes exposure less visible and response more urgent.
Evidence‑Based Policy Priorities
CDC’s 2024 analysis states that prevention efforts focused on illegally manufactured fentanyls overall will also be effective for carfentanil, while noting that more naloxone and faster response may be required. The most defensible public health priorities are:
- Expand naloxone distribution
- Distribute multiple standard‑dose naloxone units
- Train people who use drugs, friends, and family
- Improve overdose surveillance and toxicology reporting
- Rapidly communicate local alerts
- Increase access to medications for opioid use disorder
- Support supervised consumption and other harm‑reduction services where available
Why Standard‑Dose Naloxone Saturation Matters?
A notable contribution from recent literature is the argument that newer high‑dose naloxone formulations are less essential than widespread distribution of multiple standard doses.
Researchers argue for providing at least four standard intranasal or intramuscular doses rather than relying on expensive high‑dose formulations with less evidence and greater risk of precipitated withdrawal.
In public health terms, coverage beats concentration. More people carrying more standard naloxone doses is likely more valuable than fewer people carrying premium high‑dose products.
Treatment, Recovery, and Long‑Term Response
Naloxone saves lives, but it does not treat opioid use disorder or eliminate future carfentanil exposure risk. Long‑term prevention depends on linkage to care.
CDC and broader treatment literature emphasize access to treatment for substance use disorder, especially medications for opioid use disorder, as central to sustained reductions in overdose deaths.
Why Medications for Opioid Use Disorder Matter?
In a heroin‑to‑fentanyl‑to‑adulterant environment, the key overdose risk is not only intentional high‑risk use but exposure to an unstable illicit supply.
Treatment with evidence‑based medications such as buprenorphine or methadone reduces contact with that supply and therefore reduces exposure to hidden carfentanil.
Recommended Post‑Overdose Priorities
- Medical evaluation after overdose
- Offer or initiate medications for opioid use disorder when appropriate
- Harm‑reduction counseling
- Naloxone refill or resupply
- Education for household and friends
- Assessment for co‑occurring sedative use or adulterant exposure
- Referral to ongoing treatment and support services
Concrete Conclusions
After synthesizing the strongest and most current evidence, the following conclusions are warranted:
Carfentanil is a real and reemerging U.S. overdose threat. It remains rarer than fentanyl overall, but the sevenfold increase in deaths with carfentanil detected from early 2023 to early 2024 is too large to dismiss as noise.
The current carfentanil threat is mainly a hidden adulteration problem. With roughly 87% illegally manufactured fentanyl co‑detection, carfentanil is now usually embedded in fentanyl supply rather than operating as a clearly separate market.
Carfentanil overdose looks like severe opioid overdose, not a wholly distinct syndrome. The most important signs are unresponsiveness, respiratory depression, cyanosis, pinpoint pupils, hypoxia, and inability to awaken the person.
Naloxone works on carfentanil, but repeated dosing is often needed. The evidence does not support the myth that carfentanil is naloxone resistant. It does support the practical expectation that more doses may be required, often three or more.
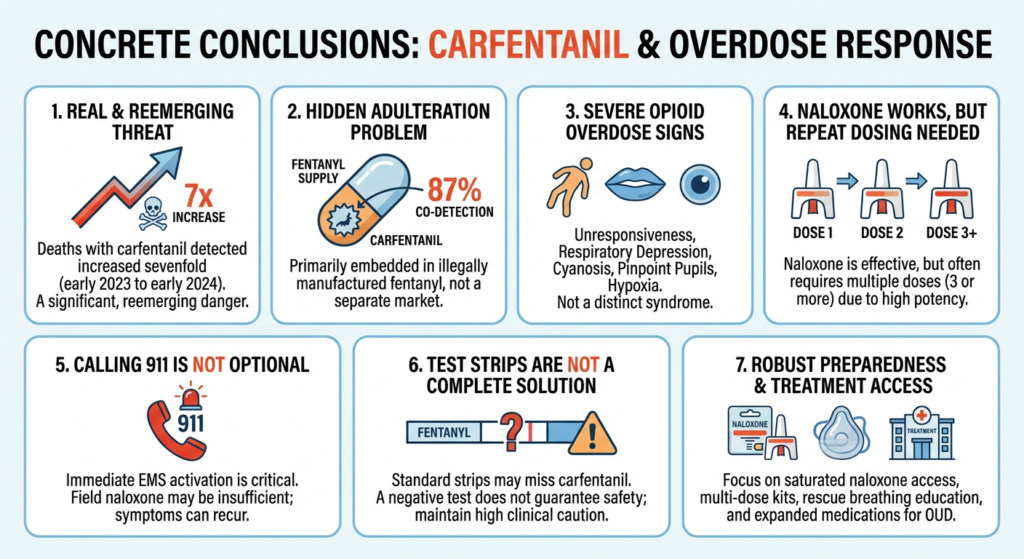
Calling 911 immediately is not optional. Field naloxone may be insufficient, symptoms may recur, and mixed‑adulterant exposures may complicate recovery.
Standard fentanyl test strips do not solve the carfentanil problem. They may miss carfentanil, so clinical caution must remain high even when a strip is negative.
The best way to reduce carfentanil deaths is not drug‑specific panic, but robust opioid overdose preparedness and treatment access. That means saturated naloxone access, multi‑dose kits, rescue‑breathing education, rapid EMS activation, local alerts, and expanded medications for opioid use disorder.
Get Help Today!
If you or someone you care about is struggling with opioid use, you don’t have to face it alone. Thoroughbred Wellness & Recovery offers compassionate, evidence‑based treatment for substance use and co‑occurring mental health disorders in a supportive environment.
Our team is available 24/7 to answer your questions and guide you toward lasting freedom. Contact our team to learn more about our programs and take the first step toward recovery.








