

Cocaine overdose is not simply a matter of taking too much. A person can experience life-threatening toxicity from cocaine through multiple pathways: rapid cardiovascular collapse, severe hyperthermia, seizures, stroke, or arrhythmia, often within seconds to minutes of use.
The most dangerous reality is that cocaine’s lethal effects are fundamentally unpredictable at the individual level because toxicity emerges from the interaction of dose, route, metabolism, alcohol co-use, hidden adulterants like fentanyl, and underlying health vulnerabilities.
This article explains how cocaine overdose happens, what signs to watch for, and what steps can save a life.
What Makes Cocaine Overdose Possible?
Cocaine acts as both a powerful stimulant and a cardiac toxin. It blocks the reuptake of catecholamines like norepinephrine and dopamine, flooding the nervous system with signals that drive heart rate, blood pressure, body temperature, and agitation to dangerous extremes.
At the same time, cocaine impairs electrical conduction in the heart through sodium channel blockade, setting the stage for life-threatening arrhythmias and sudden cardiac arrest.
The result is a toxidrome where the cardiovascular system, brain, and thermoregulatory mechanisms can all fail at once.
Death may occur from coronary vasospasm, ventricular fibrillation, intracranial hemorrhage, hyperthermic organ failure, or respiratory collapse, often while the person is still awake and agitated rather than sedated or unconscious.
Why Dose Alone Does Not Predict Overdose?
One of the most important scientific truths about cocaine toxicity is that there is no universally safe dose.
Some individuals have died from amounts far below average lethal benchmarks, while others tolerate much larger exposures. This unpredictability arises from several interacting factors:
- Route of administration changes how quickly cocaine reaches the brain and how much is converted to active metabolites
- Purity and contamination vary widely in street cocaine, especially with fentanyl adulteration
- Alcohol co-use creates cocaethylene, a longer-lasting and more cardiotoxic metabolite
- Underlying cardiac or neurologic disease may be silent until cocaine exposes the vulnerability
- Tolerance to subjective effects does not reliably protect against lethal cardiovascular or hyperthermic complications
- Repeated dosing during binges stacks physiologic stress before prior doses clear
The convergence of these variables means that overdose risk cannot be reduced to a simple milligram threshold.
How Alcohol Changes Cocaine Toxicity?
When cocaine and alcohol are used together, the liver produces cocaethylene, a psychoactive metabolite with similar behavioral effects to cocaine but a longer plasma half-life of about two hours compared to cocaine’s one hour.
Human studies show that approximately 17 to 24 percent of cocaine is converted to cocaethylene when ethanol is present, with the proportion varying by route of administration.
Cocaethylene intensifies subjective intoxication and cardiovascular stress. Users report greater liking and greater total intoxication after the cocaine-alcohol combination than after either drug alone, which can promote repeated dosing.
Meanwhile, cocaethylene prolongs active toxicity and is associated with greater concern for cardiovascular injury than cocaine alone.
Older review literature reports an 18 to 25-fold increase in risk of immediate death when cocaine and alcohol are combined, a figure that appears consistently across cocaethylene research.
The practical implication is clear: concurrent alcohol use is one of the most underappreciated biological multipliers of cocaine overdose risk.
This is not simply because users become more impaired behaviorally, but because ethanol creates an additional active toxicant that persists longer and intensifies cardiovascular danger.
Recognizing the Signs of Cocaine Overdose
Cocaine overdose often begins with signs of extreme sympathetic nervous system activation rather than sedation or unconsciousness. Early manifestations include:
- Severe agitation, paranoia, or hallucinations
- Rapid heart rate and dangerously high blood pressure
- Dilated pupils
- Profuse sweating
- Chest pain or palpitations
- Elevated body temperature
- Headache and confusion
As toxicity progresses, more severe complications emerge:
- Seizures
- Arrhythmias or irregular heartbeat
- Stroke symptoms such as weakness, facial droop, or severe headache
- Hyperthermia with core temperatures that can become extreme
- Altered mental status or loss of consciousness
- Respiratory distress or irregular breathing
- Cardiovascular collapse
The most dangerous presentations include excited delirium, characterized by extreme agitation, hyperthermia, unusual strength, and risk of sudden death, and cocaine-associated chest pain, which may reflect coronary vasospasm or true myocardial infarction even in young adults without traditional heart disease risk factors.
Stages of Acute Cocaine Toxicity
Medical references describe a three-stage progression, though patients may move rapidly between stages or skip stages entirely:
Stage 1: Early sympathetic activation
Headache, nausea, dilated pupils, twitching, increased blood pressure, rapid breathing, hyperthermia, paranoia, aggression, and agitation.
Stage 2: Established severe toxicity
Encephalopathy, seizures, increased reflexes, hypertension, arrhythmias, gasping or irregular breathing, and persistent hyperthermia.
Stage 3: Terminal decompensation
Coma, fixed and dilated pupils, loss of vital functions, hypotension, ventricular fibrillation, cardiac arrest, apnea, and respiratory failure.
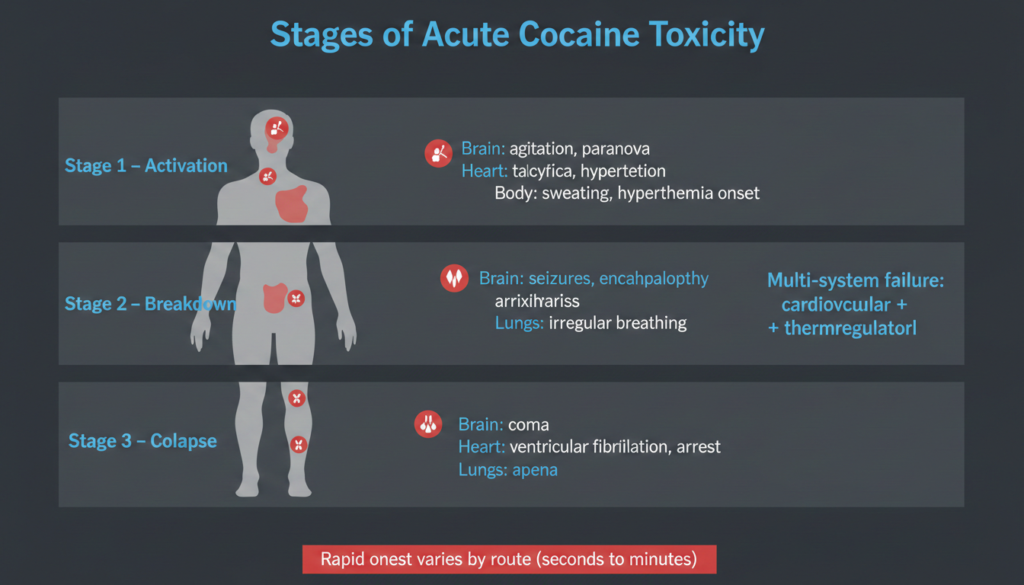
The transition between these stages may be rapid, particularly after smoked or intravenous use. Effects can appear within three to five seconds when inhaled, 10 to 60 seconds when injected intravenously, and four to five minutes when snorted.
Why Cocaine Overdose is Unpredictable?
The deeper scientific reason cocaine overdose remains unpredictable is not ignorance of cocaine’s mechanisms, but rather the convergence of well-understood mechanisms inside highly variable real-world conditions.
Cocaine’s most lethal effects are cardiovascular, but the pathway to death is shaped by factors that clinicians and users often cannot measure in real time.
The Role of Polysubstance Exposure
Real-world cocaine overdose science must be built around interaction, not isolated drug models. Forensic data show that most cocaine-related deaths involve multiple drugs. In one New York City postmortem dataset of cocaethylene-positive cases, opioids were present in 96.9 percent of cases, with fentanyl especially common.
This pattern links cocaethylene research with the modern overdose crisis: many cocaine overdoses are better understood as cocaine-centered mixed toxic syndromes.
The CDC explicitly notes that drugs including cocaine and methamphetamine may be mixed with fentanyl, which changes both recognition and response strategies because respiratory depression may indicate opioid involvement rather than pure stimulant toxicity.
Individual Vulnerability and Hidden Disease
A person may have undiagnosed structural heart disease, channelopathy, hypertension, cerebrovascular fragility, or coronary disease. Cocaine’s acute vasoconstrictive and arrhythmogenic effects can expose those vulnerabilities suddenly.
This contributes to the apparent randomness of overdose: some users survive many exposures, while another suffers fatal dysrhythmia or stroke after a smaller dose.
Tolerance to some effects develops with chronic use, but tolerance is incomplete and uneven. Users may interpret tolerance as safety, yet tolerance to euphoria or certain hemodynamic responses does not ensure protection from coronary vasospasm, arrhythmia, stroke, hyperthermia, cocaethylene-mediated risk, or fentanyl contamination.
What to Do If You Suspect Cocaine Overdose?
Immediate action can save a life. Call emergency services right away if any of the following are present:
- Chest pain
- Seizure
- Severe agitation, confusion, or delirium
- Very high body temperature with profuse sweating
- Collapse, syncope, or unresponsiveness
- Trouble breathing, cyanosis, or irregular breathing
- Signs of stroke such as weakness, facial droop, severe headache, or speech changes
While waiting for emergency responders:
- Keep the person as calm and cool as possible
- Avoid escalating confrontation
- If unresponsive but breathing, place in the recovery position
- If not breathing normally, follow emergency dispatcher instructions and provide rescue breathing or CPR as directed
- If opioid contamination is possible and naloxone is available, give naloxone when the person is unresponsive or breathing poorly
Naloxone will not reverse cocaine itself, but it can reverse opioid effects if fentanyl or another opioid is present. The CDC notes that naloxone can reverse an opioid overdose and should be widely available, even among people who use stimulants.
Do not assume the person will “sleep it off.” Do not delay calling because the person is still awake. Violent agitation, chest pain, seizure, or overheating after cocaine use are emergency signs even if the person is still conscious.
Medical Treatment for Cocaine Overdose
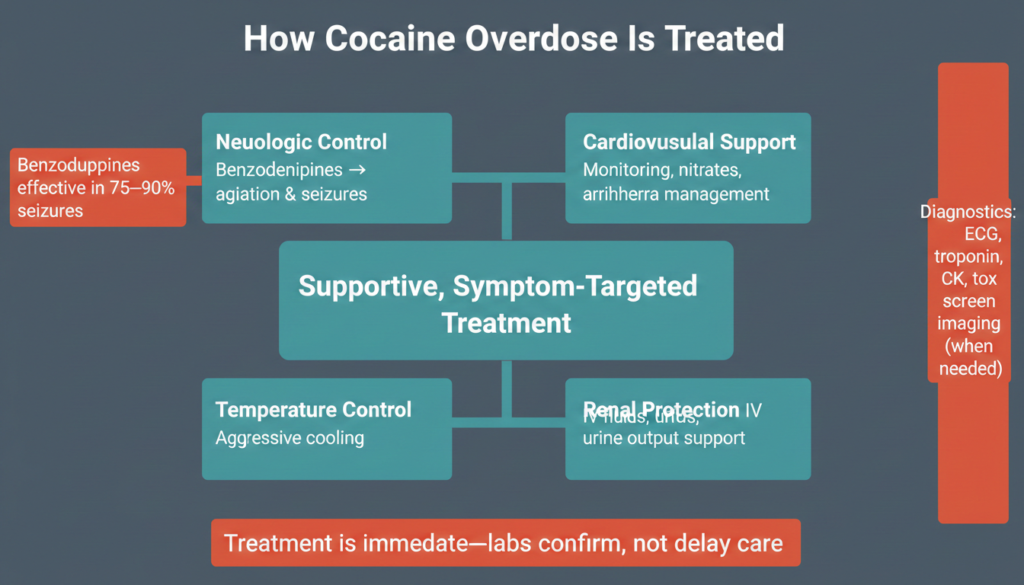
There is no specific antidote for cocaine toxicity. Management is supportive and targets complications as they emerge. Emergency treatment typically includes:
- Airway support and oxygen as needed
- Intravenous access and cardiac monitoring
- Benzodiazepines for agitation and seizures, which are first-line therapy and reportedly effective in 75 to 90 percent of cocaine-induced seizures
- Aggressive cooling measures for hyperthermia
- Fluids to maintain urine output and mitigate rhabdomyolysis-associated renal injury
- Nitrates, aspirin, and other agents for chest pain and acute coronary syndrome
- Sodium bicarbonate for QRS widening and ventricular arrhythmias related to sodium channel blockade
Physical restraint should be avoided if possible because it may worsen rhabdomyolysis and hyperthermia. Beta-blockers are generally avoided in acute cocaine toxicity due to concern for unopposed alpha stimulation, which can worsen vasoconstriction and hypertension.
Evaluation in the emergency department may include ECG, troponin, creatine kinase, renal and hepatic function tests, urinalysis, urine toxicology screen, chest imaging, and head CT when indicated. However, clinical recognition and treatment should not wait for laboratory confirmation.
Long-Term Risks and Recovery
Cocaine use carries serious long-term health risks beyond acute overdose. Chronic use can lead to:
- Cardiovascular disease including cardiomyopathy and increased risk of heart attack and stroke
- Neurologic damage including cognitive impairment and movement disorders
- Nasal and sinus damage from snorting
- Lung injury from smoking
- Infectious disease risk from injection use
- Mental health complications including anxiety, depression, and psychosis
Recovery from cocaine use disorder is possible with comprehensive treatment. Evidence-based approaches include behavioral therapies such as cognitive behavioral therapy and contingency management, along with treatment for co-occurring mental health conditions.
While there are currently no FDA-approved medications specifically for cocaine use disorder, research continues in this area.
The Bottom Line
Cocaine overdose is unpredictable because toxicity is generated by interacting systems, not dose alone. Those systems are destabilized further by alcohol-derived cocaethylene, route-specific exposure patterns, hidden co-ingestants like fentanyl, and large differences in host vulnerability.
The most lethal effects are usually cardiovascular, but neurologic and thermoregulatory complications are equally capable of precipitating collapse.
The most clinically important skill in cocaine overdose is recognizing that agitated, sweating, hypertensive, hot, and irrational behavior is already a potentially life-threatening overdose pattern, not a precursor to one.
Waiting for unconsciousness or respiratory arrest means responding late to a syndrome that has already advanced to severe neurologic, cardiac, or metabolic injury.
If you or someone you know is struggling with cocaine use, professional help is available. Thoroughbred Wellness & Recovery offers comprehensive dual diagnosis treatment that addresses both substance use and co-occurring mental health conditions through evidence-based and holistic approaches. Call 770-564-4856 to speak with a compassionate team member 24/7.








