

When you’re searching for mental health and addiction treatment, the terms you encounter, dual diagnosis, co-occurring disorders, comorbidity, concurrent disorders, can feel like a maze.
You might wonder if these labels mean the same thing or if choosing the wrong one will send you to the wrong program. The truth is simpler than the jargon suggests: all these terms describe having both a mental health condition and a substance use disorder at the same time.
What matters most is finding a provider who treats both conditions together, not the exact label they use. This article will clarify the differences, explain why the terminology debate exists, and show you how to navigate insurance and treatment options with confidence.
What Dual Diagnosis and Co-Occurring Disorders Really Mean?
The U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) defines co-occurring disorders as the presence of at least one mental health disorder and at least one substance use disorder in the same person.
This definition is intentionally broad because there are no special or unique combinations that define co-occurrence. You might have depression and alcohol use disorder, PTSD and opioid dependence, or bipolar disorder and stimulant addiction. Each pairing is valid and requires integrated care.
“Dual diagnosis” is an older term that became popular in the 1980s and 1990s to describe the same reality. It entered clinical programs and research to signal that someone had both a serious mental illness and a substance use disorder.
The phrase stuck in marketing and everyday conversation, but it has a subtle problem: “dual” implies exactly two disorders, which can be misleading when someone has multiple mental health conditions or uses several substances.
SAMHSA’s shift to “co-occurring disorders” was deliberate. The agency wanted to avoid implying “only two” and to clarify that each disorder must be established independently, not just as a symptom of the other.
For example, if your anxiety only appears when you’re intoxicated and disappears when you’re sober, that’s substance-induced anxiety, not a co-occurring disorder. True co-occurrence means both conditions exist on their own and influence each other.
Why the Labels Vary Across Organizations?
International bodies and professional groups use different terms, which adds to the confusion. The World Health Organization and the European Monitoring Centre for Drugs and Drug Addiction have historically used “dual diagnosis” and “comorbidity” interchangeably, sometimes even applying “dual diagnosis” to any two psychiatric disorders.
The World Association on Dual Disorders advocates for “dual disorder” as a unified term to reduce stigma and support research that views the conditions as a single complex problem rather than two separate issues.
In the United States, the American Society of Addiction Medicine (ASAM) uses “dual diagnosis” and “co-occurring disorders” variably across its criteria documents.
This inconsistency isn’t just academic. It shapes how treatment programs describe themselves, how insurance companies write policies, and how professionals assess and place patients.
Comorbidity vs Dual Diagnosis: A Subtle but Important Distinction
“Comorbidity” is a general medical term for having multiple conditions at the same time. It’s used across all of healthcare to describe patients with, say, diabetes and heart disease or chronic kidney disease and anemia. In behavioral health, comorbidity can refer to any combination of mental health and substance use disorders, but it doesn’t carry the same clinical specificity as “dual diagnosis” or “co-occurring disorders.”
Insurance companies and payment systems use comorbidity to refine case-mix and estimate resource use. When a plan frames your case as general comorbidity, it may push you into separate treatment tracks, one for mental health, another for substance use, rather than recognizing that you need integrated care. This framing can lead to fragmented services, duplicated assessments, and authorization delays.
In contrast, when providers use “dual diagnosis” or “co-occurring disorders,” they signal that your mental health and substance use conditions are intertwined and require coordinated treatment. This framing supports billing for integrated services like the Collaborative Care Model and behavioral health integration codes, which Medicare and many private payers now reimburse.
Concurrent Disorders: The Canadian and International Perspective
“Concurrent disorders” is the preferred term in Canada and some other countries. It means the same thing as co-occurring disorders: having a mental health disorder and a substance use disorder at the same time.
The Canadian Centre on Substance Use and Addiction and provincial health systems use this language in their clinical guidelines and public health campaigns.
If you’re researching treatment or reading international literature, you’ll see “concurrent disorders” frequently. It’s not a different clinical concept, just a regional preference.
The important takeaway is that all these terms, dual diagnosis, co-occurring disorders, concurrent disorders, and comorbidity, point to the same need: integrated treatment that addresses both your mental health and substance use together.
Why Terminology Confusion Creates Real Treatment Gaps?
The lack of a single standard term has real-world consequences. Professionals who don’t know which label to use when ordering assessments, drafting prior authorization requests, or coding for reimbursement can inadvertently trigger denials or delays. Here’s how the confusion plays out:
- Assessment inconsistency: A primary care doctor refers you for “dual diagnosis IOP,” but the treatment center’s intake form asks about “co-occurring disorders,” and the insurance portal lists “comorbid mental health and SUD.” Each system expects different documentation, and missing the right keyword can stall your admission.
- Fragmented care: When a plan treats your case as general comorbidity, it may require separate authorizations for mental health therapy and substance use counseling, forcing you to see different providers in different locations. This violates the integrated care model that evidence supports.
- Coding errors: Billing staff who document “dual diagnosis” in narrative notes but fail to assign specific ICD-10-CM codes for both the mental disorder and the substance use disorder can generate claim denials. Payers don’t recognize “dual diagnosis” as a billable diagnosis; they need precise codes like F33.1 for major depressive disorder, recurrent, moderate, and F10.20 for alcohol dependence.
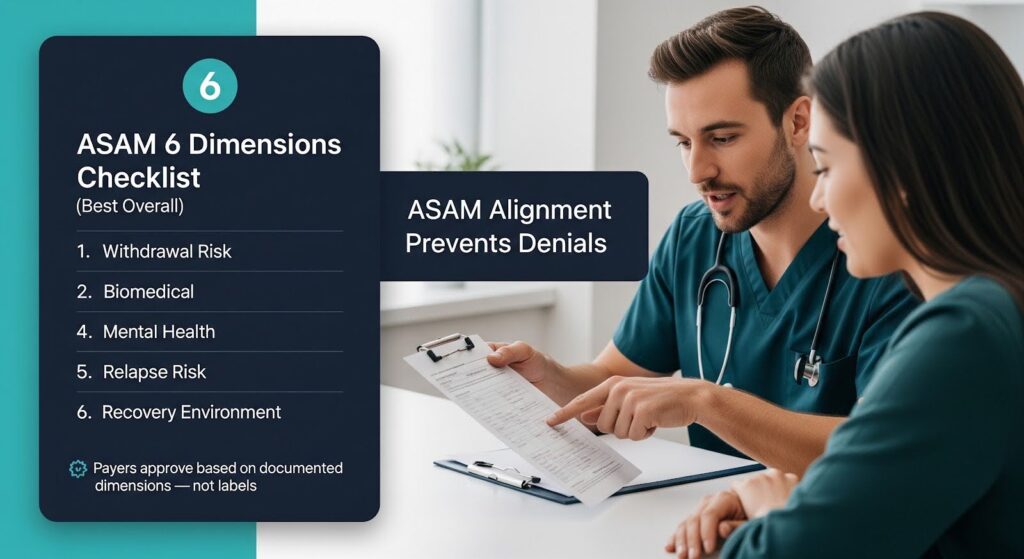
- Authorization denials: Insurance reviewers trained on ASAM criteria expect documentation using ASAM’s six dimensions (withdrawal risk, biomedical conditions, emotional/behavioral issues, readiness to change, relapse potential, and recovery environment). If your provider’s request uses “dual diagnosis” language without mapping to ASAM dimensions, the reviewer may deny the request as not meeting medical necessity.
A systematic review of randomized controlled trials on dual diagnosis treatment found that integrated care, where the same team treats both conditions concurrently, tends to produce significantly greater reductions in psychiatric symptoms, especially PTSD, compared to non-integrated care.
Yet the review also noted that terminology ambiguity and inconsistent service definitions across studies made it harder to compare outcomes and implement best practices.
How Insurance Companies Use Labels to Control Coverage?
Insurance plans operationalize these labels through utilization management (UM) tactics: prior authorization, internal coverage criteria, and nonquantitative treatment limitations (NQTLs).
The 2024 Medicare Advantage prior authorization reforms and the 2024 final mental health parity rules have narrowed some of these tactics, but gaps remain.
Prior Authorization and Medical Necessity
Medicare Advantage plans must now limit prior authorization to confirming diagnoses and ensuring medical necessity.
Approvals must remain valid as long as medically necessary, and plans must provide a 90-day transition period without new prior authorization when you switch plans mid-treatment. Despite these protections, plans still exploit documentation ambiguities.
For example, if your provider bills psychotherapy add-on with an evaluation and management (E/M) visit (CPT code 90833) but doesn’t clearly document that the psychotherapy and medical management were significant and separately identifiable, the claim will be denied as “not separately identifiable.”
This denial pattern is common in co-occurring disorder treatment, where a single visit might include medication management for depression and psychotherapy for trauma related to substance use.
Internal Coverage Criteria and ASAM Alignment
Most major payers, Optum/UnitedHealthcare, Cigna, Aetna, and many Blue Cross plans, have adopted ASAM Criteria as the national framework for substance use disorder levels of care.
State laws in North Carolina, Maryland, Illinois, and West Virginia require commercial plans to use ASAM for placement decisions.
ASAM doesn’t mandate a specific term like “dual diagnosis” or “co-occurring disorders,” but it does require documentation across six dimensions.
If your provider writes “dual diagnosis IOP” without detailing your relapse history, recovery environment risks, or emotional/behavioral conditions, the utilization reviewer may deny the request even though you clearly need integrated care.
The Parity Enforcement Opportunity
The 2024 final mental health parity rules prohibit plans from using processes, strategies, or evidentiary standards for mental health and substance use benefits that are more stringent than those for medical/surgical benefits.
Plans must conduct documented comparative analyses showing that their NQTLs are comparable and not discriminatory.
If your plan denies integrated co-occurring disorder treatment by splitting your care into separate mental health and SUD tracks, while allowing integrated care for medical conditions like diabetes with kidney disease, you can challenge that denial under parity.
The plan must prove its UM processes are comparable, and it must collect and review outcomes data to ensure its NQTLs don’t worsen access.
Coding and Documentation: The Technical Side of the Label Problem
Behind every label is a set of codes that determine payment. The U.S. healthcare system uses ICD-10-CM diagnosis codes and CPT/HCPCS procedure codes. Neither “dual diagnosis” nor “co-occurring disorders” appears as a billable code. Instead, providers must assign specific codes for each condition and link them to the services billed.
ICD-10-CM Diagnosis Sequencing
Your medical record should list both your mental health disorder (for example, F33.1 for major depressive disorder, recurrent, moderate) and your substance use disorder (for example, F11.20 for opioid dependence). The order matters: the primary diagnosis should reflect the main focus of the visit, and secondary diagnoses capture other active conditions.
Payers use diagnosis sequencing to validate medical necessity. If you’re billed for psychotherapy but only the substance use disorder is listed, the claim may be denied because psychotherapy typically requires a mental health diagnosis. Conversely, if you’re in an opioid treatment program and the claim omits the opioid use disorder diagnosis, it will be rejected.
CPT/HCPCS Codes for Integrated Care
Medicare and many private payers reimburse integrated behavioral health services through specific codes:
- CPT 99484 (general behavioral health integration) and 99492–99494 (psychiatric Collaborative Care Model) describe monthly team-based services with a behavioral health care manager and psychiatric consultant.
- HCPCS G2214 was created in 2021 to capture shorter-interval Collaborative Care when the usual monthly time thresholds aren’t met, addressing a common denial pattern for patients who are hospitalized or referred mid-month.
- Psychotherapy add-on with E/M (CPT 90833) requires documentation showing both the psychotherapy and the medical management were significant and separately identifiable, with total time recorded.
Opioid treatment programs (OTPs) have their own billing rules. Every OTP claim must include an opioid use disorder diagnosis, use place of service code 58, and append telehealth modifiers (95 for audio-video, 93 for audio-only) when applicable. Missing any of these elements triggers automatic denials.
The DSM-5 vs ICD-10-CM Friction
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) unified “substance abuse” and “dependence” into a single “substance use disorder” with severity levels (mild, moderate, severe) based on symptom counts.
ICD-10-CM, however, still uses an older structure that approximates abuse versus dependence. This mismatch forces a crosswalk: mild SUD maps to abuse codes, and moderate/severe SUD maps to dependence codes.
Providers often document DSM-5 severity in narrative notes but fail to translate it into the correct ICD-10-CM code. Without structured templates that count DSM-5 criteria and suggest corresponding ICD-10-CM codes, miscoding is common.
The American Psychiatric Association maintains an updated portal for DSM–ICD-10-CM code changes, with 2025 updates effective October 1, 2025.
What the Evidence Says About Integrated vs Non-Integrated Care?
The clinical case for integrated treatment is strong. A synthesis of randomized trials from 2009 to 2018 found that integrated treatment tends to yield significantly greater reductions in psychiatric symptoms, especially PTSD, compared to non-integrated care.
Substance use outcomes and treatment retention were comparable between integrated and non-integrated models in some trials, but integrated care remained the preferred standard due to symptom reductions, patient satisfaction, lower acute care utilization, and cost-effectiveness.
SAMHSA reports that approximately 21.2 million adults had co-occurring mental illness and substance use disorder in 2024. The scale of need and the bidirectional influence of these conditions, where one disorder often worsens or maintains the other, support the rationale for integrated care that addresses both together.
Early integrated program research in the 1990s showed effectiveness but also highlighted risks. Some psychiatric-first settings undertreated substance use while overtreating psychiatric symptoms, underscoring the need for balanced, competency-based integrated teams. Modern integrated models like the Collaborative Care Model address this by requiring psychiatric consultation, measurement-based care, and care manager coordination.
Practical Strategies to Navigate the Label Problem
You don’t need to become a coding expert, but understanding a few key strategies can prevent denials and delays.
Ask Your Provider to Use “Co-Occurring Disorders” in Documentation
When your provider writes referrals, prior authorization requests, and clinical notes, ask them to use “co-occurring disorders” or “COD” rather than “dual diagnosis.”
This aligns with SAMHSA’s standard and signals to payers that you need integrated care. The documentation should explicitly state that you have at least one mental health disorder and at least one substance use disorder, each established independently.
Ensure ASAM Dimensions Are Documented
If you’re seeking intensive outpatient (IOP), partial hospitalization (PHP), residential, or detox services, your provider’s authorization request should address all six ASAM dimensions with specific evidence.
For example, “Dimension 5 (relapse potential): multiple relapses despite prior IOP; failed to maintain abstinence in non-24-hour settings; residential level indicated to interrupt high-risk environment.”
Verify Coding Accuracy
Ask your billing staff to confirm that both your mental health and substance use diagnoses are coded on every claim and linked to the services billed. For integrated visits, ensure psychotherapy time and E/M decision-making are documented separately, and that total time is recorded.
For opioid treatment, verify that place of service 58 and the opioid use disorder diagnosis are on every claim.
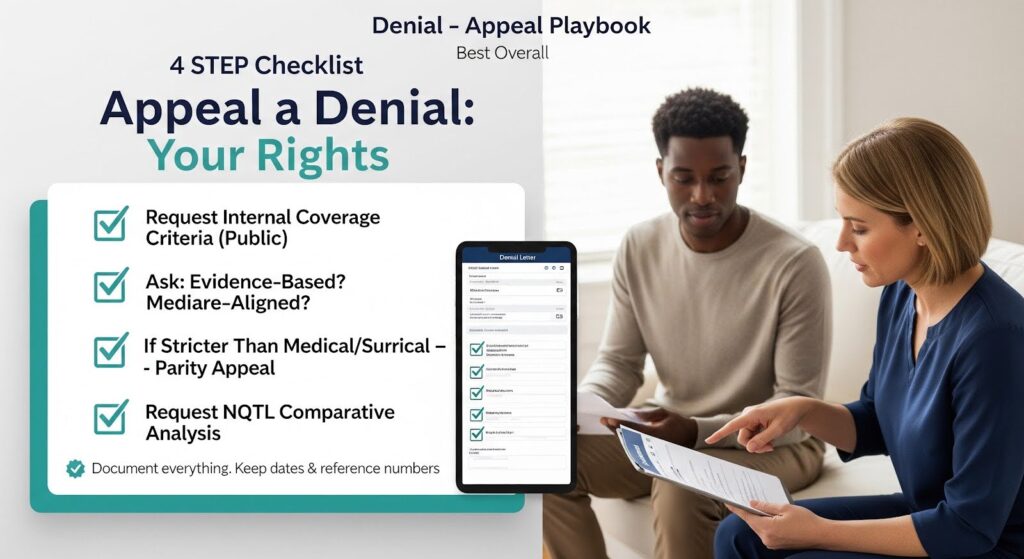
Use Your Appeal Rights
If your claim is denied, request the plan’s internal coverage criteria and demand that it be publicly accessible and evidence-based. Under the 2024 Medicare Advantage rules, plans must make internal criteria available to the public, not behind paywalls.
If the criteria diverge from Traditional Medicare coverage or apply more stringent standards to mental health and substance use than to medical/surgical services, challenge the denial under parity.
For Medicare Advantage, cite the 90-day transition period if you switched plans mid-treatment, and assert that prior authorization approvals must remain valid as long as medically necessary.
For all plans, request the documented comparative analysis showing that the plan’s utilization management for co-occurring disorder treatment is comparable to its UM for integrated medical conditions.
The Path Forward: A Clear Position on Labels and Coverage
Based on the regulatory and clinical evidence, my position is clear: in 2026, when a plan uses “comorbidity” labeling to splinter or deny integrated mental health and substance use treatment, that approach conflicts with federal policy.
The 2024 Medicare Advantage prior authorization reforms limit prior authorization to necessary clinical verifications and require continuity. The 2024 parity NQTL rules explicitly prohibit discriminatory processes and demand comparability, transparency, and outcomes accountability.
CMS payment policies for the Collaborative Care Model, behavioral health integration, and opioid treatment programs operationalize integrated care. The creation of HCPCS G2214 neutralized a common denial tactic related to time thresholds.
Opioid treatment program billing rules clarify place of service, telehealth modifiers, and multi-OTP scenarios, further limiting technical denials.
The clinically accurate “dual diagnosis” or “co-occurring disorders” frame, implemented via precise ICD-10-CM sequencing and integrated CPT/HCPCS coding, should prevail in coverage determinations.
However, compliance is not automatic. Plans continue to exploit documentation gaps, technical coding lapses, and opaque internal criteria.
The path to coverage runs through three disciplines: impeccable integrated coding and documentation, assertive application of Medicare Advantage prior authorization rights and parity NQTL demands, and strategic use of Collaborative Care Model, behavioral health integration, and opioid treatment program codes calibrated to real-world intervals and modalities.
When providers rigorously implement this approach, denials predicated on “the label” become indefensible, and integrated care becomes not only clinically necessary but also administratively inescapable under federal rules.
Why It Matters: Real Outcomes for Real People
The terminology debate isn’t just about words. It’s about whether you receive coordinated care from a team that understands how your depression fuels your drinking, or whether you’re shuttled between a therapist who won’t discuss your substance use and a counselor who won’t address your trauma.
It’s about whether your insurance approves 30 days of residential treatment or denies it because the request didn’t use the right ASAM language. It’s about whether your opioid treatment program can bill for telehealth counseling or whether a missing modifier triggers a recoupment.
Approximately 21.2 million adults need integrated care for co-occurring mental health and substance use disorders. The evidence supports integrated treatment.
Federal policy increasingly mandates it. Yet the label problem persists, creating avoidable gaps for professionals and patients who don’t know what to ask for.
The solution is not to wait for the field to settle on a single term. The solution is to understand that “dual diagnosis,” “co-occurring disorders,” “concurrent disorders,” and “comorbidity” all describe the same clinical reality, and to ensure that your documentation, coding, and appeals leverage the regulatory protections now in place. When you do, the label becomes less important than the care you receive.
If you or someone you care about is navigating co-occurring mental health and substance use challenges, don’t let terminology confusion delay treatment.
Reach out to a provider who offers integrated care, verify that your insurance will cover it, and advocate for the coordinated services you deserve. Your recovery depends on it.
Need integrated treatment for co-occurring mental health and substance use disorders? Contact Thoroughbred Wellness & Recovery to learn how our dual diagnosis programs can support your path to lasting freedom.








