

Quitting marijuana after heavy use can feel overwhelming, especially when sleep disappears and irritability spikes.
Most heavy daily users experience withdrawal symptoms that begin within 24 to 48 hours, peak around days 2 to 6, and largely resolve within 2 to 3 weeks, though sleep disturbances often persist for 4 to 6 weeks.
This article explains what to expect during marijuana detox, how long symptoms last, and what evidence-based strategies can help you get through it.
What is Marijuana Withdrawal Syndrome?
Cannabis withdrawal syndrome is a recognized medical condition included in the DSM-5, the standard diagnostic manual used by mental health professionals.
It occurs when someone who has used marijuana heavily or daily for an extended period suddenly stops or significantly reduces their use.
The syndrome includes a cluster of symptoms: irritability or anger, anxiety, sleep difficulty including vivid dreams, decreased appetite or weight loss, restlessness, depressed mood, and at least one physical symptom such as abdominal pain, tremors, sweating, fever, chills, or headache.
These symptoms must cause clinically significant distress or impairment and cannot be better explained by another medical or psychiatric condition.
Research shows that cannabis withdrawal is common, affecting about 47% of regular or dependent users in pooled analyses of more than 20,000 individuals.
Rates vary by setting: community samples report around 17%, outpatient clinical samples around 54%, and inpatient clinical samples as high as 87%.
The higher rates in treatment settings reflect the fact that people seeking help typically have more severe patterns of use and greater symptom burden.
How Long Does Marijuana Detox Take?
The timeline for marijuana detox follows a predictable pattern for most heavy users, though individual experiences vary based on frequency of use, potency of products, and personal factors.
Onset: 24 to 48 Hours
Withdrawal symptoms typically begin within one to two days after your last use. You may notice early signs like restlessness, mild anxiety, or difficulty falling asleep.
Appetite may start to decrease, and some people report feeling irritable or on edge.
Peak: Days 2 to 6
Most symptoms reach their highest intensity between days 2 and 6 after cessation. This is when irritability, anxiety, insomnia, and mood changes are most pronounced.
Sleep disruption becomes especially noticeable during this window, with many people experiencing prolonged time to fall asleep, frequent awakenings, and vivid or disturbing dreams.
Resolution: 2 to 3 Weeks for Most Symptoms
For many heavy daily users, the majority of withdrawal symptoms substantially improve within 2 to 3 weeks.
Mood stabilizes, appetite returns, and daytime functioning improves. However, this timeline can extend in people with very heavy use patterns, those who used high-potency concentrates, or individuals with co-occurring mental health conditions.
The Long Tail: Sleep Disturbances Up to 6 Weeks
Sleep problems are often the last symptoms to resolve. Insomnia and abnormal dreams can persist for 30 to 45 days or longer in some cases.
Objective sleep studies using polysomnography show that cannabis withdrawal decreases sleep efficiency and total sleep time while increasing REM sleep and shortening REM latency, a pattern that takes weeks to normalize.
Common Marijuana Withdrawal Symptoms
Understanding what you might experience can help you prepare and recognize that these symptoms are temporary and part of the recovery process.
- Irritability and anger: One of the most common complaints, often peaking in the first week and gradually subsiding.
- Anxiety and restlessness: Feelings of nervousness, tension, or being on edge are frequent during early withdrawal.
- Insomnia and vivid dreams: Sleep disruption is both common and functionally impairing, often driving relapse attempts.
- Depressed mood: Low mood, lack of motivation, or anhedonia can occur, especially in the first two weeks.
- Decreased appetite and weight loss: Many people lose interest in food during the first week, though appetite typically returns by week two.
- Physical symptoms: Abdominal discomfort, nausea, sweating, chills, headache, and tremors are generally milder than withdrawal from alcohol or benzodiazepines but still contribute to distress.
- Cravings: Urges to use cannabis can be intense, particularly in the first week, and are often triggered by environmental cues or the desire to relieve withdrawal discomfort.
These symptoms are validated by standardized assessment tools like the Marijuana Withdrawal Checklist and the Cannabis Withdrawal Scale, which clinicians use to monitor severity and guide treatment decisions.
Why Withdrawal Happens: The Neurobiology of Recovery
Chronic marijuana use downregulates cannabinoid type-1 receptors in the brain. These CB1 receptors are part of the endocannabinoid system, which regulates mood, sleep, appetite, and stress response.
When you use marijuana heavily, your brain adapts by reducing the number and sensitivity of these receptors.
When you stop using, your brain is left with a depleted receptor system and must work to restore balance. PET imaging studies using specialized tracers show that CB1 receptor availability is reduced in chronic users but begins to increase rapidly during early abstinence.
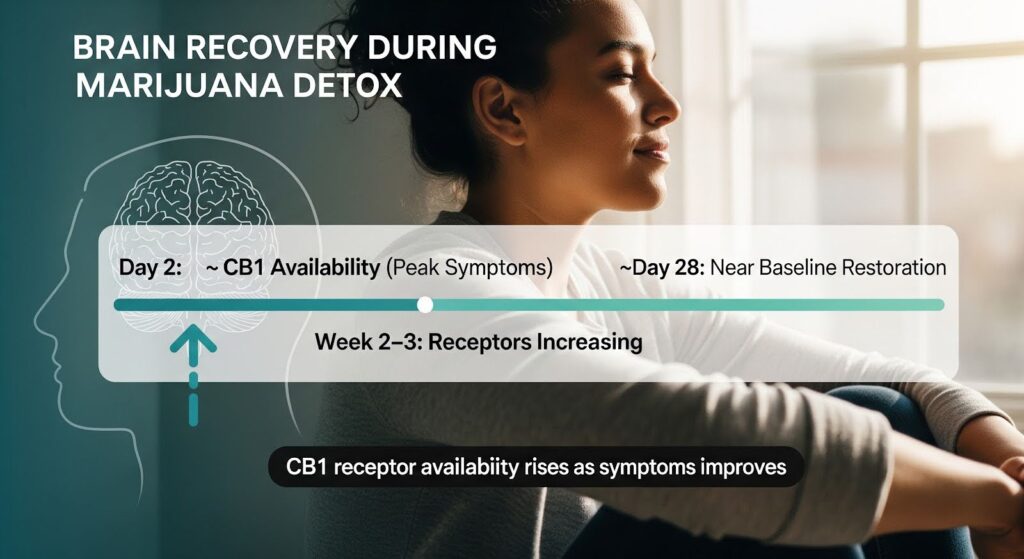
By approximately 28 days, receptor availability approaches normal baseline levels in many individuals.
This neurobiological recovery timeline closely mirrors the clinical symptom timeline. Early in abstinence, around day 2, lower CB1 receptor availability correlates with higher withdrawal severity.
As receptors recover over the following weeks, symptoms improve. This mechanism-informed understanding supports the expectation that most people will see major symptom relief within 2 to 3 weeks and near-complete normalization by 4 to 6 weeks.
Marijuana Detox Symptoms Timeline: A Week-by-Week Guide
| Time Period | What to Expect | Management Focus |
|---|---|---|
| Days 0–2 | Onset of restlessness, mild anxiety, early sleep difficulty, decreased appetite | Psychoeducation, sleep hygiene, hydration, structured daily routine |
| Days 2–6 | Peak irritability, anxiety, insomnia, vivid dreams, mood changes, physical discomfort | Coping skills, short-term sleep support if needed, frequent check-ins, relapse prevention planning |
| Days 7–14 | Gradual improvement in mood and appetite; sleep still fragile; cravings may persist | Taper any short-term medications, intensify behavioral therapy, reinforce daytime structure |
| Days 14–28 | Most acute symptoms resolve; lingering sleep abnormalities and dreams improve; relapse risk declines | Maintain psychosocial support, transition to relapse prevention focus, review triggers |
| 30–45+ Days | Sleep normalizes for most; residual symptoms rare; focus shifts to long-term recovery | Ongoing therapy, lifestyle consolidation, community support |
Factors That Influence Withdrawal Severity and Duration
Not everyone experiences withdrawal the same way. Several factors predict more severe or prolonged symptoms.
Frequency and Intensity of Use
Daily or near-daily use is consistently associated with greater withdrawal severity. The more frequently and heavily you used marijuana, the more pronounced your symptoms are likely to be.
Potency and Route of Use
High-potency cannabis products, especially concentrates like dabs, shatter, or wax, often contain 80% THC or more, compared to 10 to 25% in typical flower.
Regular use of concentrates is linked to higher tolerance and, anecdotally and observationally, more severe withdrawal experiences. This likely reflects deeper CB1 receptor downregulation from sustained high-THC exposure.
While rigorous causal studies are limited, clinical experience suggests that people who primarily used concentrates should anticipate greater symptom intensity and plan proactive support.
Tobacco Co-Use
Concurrent tobacco use is common among cannabis users and complicates withdrawal. Nicotine withdrawal overlaps with cannabis withdrawal in symptoms like irritability, anxiety, and sleep disturbance, making it harder to distinguish which substance is driving which symptom.
Tobacco co-dependence predicts more severe cannabis withdrawal and may require integrated cessation planning.
Psychiatric Comorbidity
People with co-occurring mental health conditions such as depression, anxiety, PTSD, or bipolar disorder often experience more severe withdrawal and delayed improvement.
In some studies, individuals with lifetime psychiatric illness showed withdrawal improvement delayed by approximately one week compared to those without psychiatric diagnoses. Integrated mental health care is essential for this population.
Age and Sex
Younger age is associated with greater withdrawal severity in some studies. Emerging evidence suggests that women may experience higher rates or intensity of certain symptoms, possibly due to sex-related differences in endocannabinoid system function. Tailored monitoring and support may benefit these groups.
Sleep Disruption During Marijuana Withdrawal
Sleep problems are among the most disabling aspects of cannabis withdrawal and a leading driver of relapse. Many people report using marijuana specifically to help them sleep, and when they stop, insomnia can feel unbearable.
What Happens to Sleep During Withdrawal
Objective sleep studies reveal that cannabis withdrawal decreases sleep efficiency, reduces total sleep time, and disrupts sleep architecture.
Specifically, withdrawal is associated with decreased slow-wave sleep and increased REM sleep, often with shortened REM latency. This REM rebound can lead to vivid, intense, or disturbing dreams that many people find distressing.
Subjectively, people report difficulty falling asleep, frequent awakenings, nonrestorative sleep, and nightmares. These sleep disturbances typically peak in the first week but can persist for 30 to 45 days or longer in heavy users.
Why Sleep Matters for Recovery
Poor sleep increases relapse risk, impairs daytime functioning, and worsens mood and anxiety.
Resolving insomnia early is crucial to preventing what some clinicians call “functional collapse,” where the inability to sleep undermines work, school, or family responsibilities and drives a return to use.
Evidence-Based Sleep Interventions
Behavioral strategies should be first-line. Sleep hygiene basics include maintaining a consistent wake time, getting morning light exposure, avoiding caffeine after early afternoon, limiting screen time before bed, and using the bed only for sleep.
Cognitive behavioral therapy for insomnia, or CBT-I, has shown benefit in cannabis users and can reduce both insomnia and cannabis use even when the intervention does not directly target substance use.
In controlled settings, extended-release zolpidem has been shown to normalize sleep architecture during acute cannabis withdrawal and improve sleep efficiency without next-day cognitive impairment.
A short, time-limited course of a hypnotic medication may be appropriate for selected patients with severe insomnia, alongside behavioral strategies and careful monitoring to avoid substituting one dependency for another.
Treatment Options During Marijuana Detox
There are no FDA-approved medications specifically for cannabis withdrawal, but several approaches have evidence supporting their use.
Psychosocial Interventions
Motivational enhancement therapy, cognitive behavioral therapy, and contingency management are the foundation of cannabis use disorder treatment.
These therapies help you develop coping skills, manage cravings, identify triggers, and build a relapse prevention plan. Starting these interventions early in the withdrawal period can reduce relapse risk and support long-term recovery.
Pharmacologic Support
Several medications have been studied for cannabis withdrawal, though all remain off-label.
FAAH inhibition is an investigational approach that shows promise. The drug PF-04457845 inhibits the enzyme that breaks down anandamide, a natural endocannabinoid, thereby augmenting endocannabinoid tone to buffer withdrawal.
In a randomized controlled trial, PF-04457845 significantly reduced withdrawal symptoms including depression, irritability, and anxiety, improved sleep both objectively and subjectively, and reduced cannabis use over four weeks compared to placebo.
While not yet clinically available, this mechanism-aligned strategy represents a coherent path forward.
THC agonists like dronabinol and nabilone reduce withdrawal severity in laboratory and clinical studies but have limited impact on sustained abstinence.
They carry psychoactive effects and potential for misuse, so they may be reasonable short-term bridge therapies in selected patients with severe withdrawal, coupled with a structured taper and psychosocial treatment.
Short-term hypnotics such as extended-release zolpidem can address severe insomnia during the first one to two weeks of withdrawal. Careful patient selection and monitoring are essential to avoid sedative-hypnotic dependence.
Cannabidiol is non-intoxicating and may reduce cannabis use in some studies, though its effects on acute withdrawal are less clear. Product quality variability outside clinical trials complicates translation to practice.
When is Inpatient Detox Needed?
Cannabis withdrawal rarely requires medical inpatient detoxification on its own. Most people can be managed safely and effectively in an outpatient setting with supportive care, psychoeducation, and structured follow-up.
Inpatient or higher levels of care may be indicated for individuals with severe psychiatric comorbidity such as active suicidality or psychosis, significant polysubstance withdrawal risk involving alcohol or benzodiazepines, unstable medical conditions, safety concerns like homelessness, or repeated failure to maintain abstinence in outpatient settings due to severe distress.
Managing Relapse Risk During Withdrawal
Relapse risk is highest in the first one to two weeks of abstinence, when insomnia, irritability, and anxiety peak. Targeted sleep management, contingency planning for high-risk situations like evenings or weekends, and frequent check-ins with a counselor or support network are critical during this window.
Withdrawal severity sometimes predicts later involvement severity, especially in adolescents. However, modifiable factors like sleep treatment, psychosocial support, and management of nicotine co-use shape outcomes.
Comprehensive care that addresses these factors improves the likelihood of sustained abstinence or meaningful reduction in use.
Special Populations and Considerations
Adolescents and Young Adults
Withdrawal is common and clinically meaningful in younger populations. Shorter chronicity of use may yield milder sleep changes than in adults, but early relapse remains a concern.
Family engagement, school coordination, and technology-enabled interventions such as text-based check-ins can add value.
Women
Some studies suggest women experience higher symptom counts or intensity. Proactive screening for mood, anxiety, and sleep disturbance, along with tailored coping skills and support, may benefit women during withdrawal.
Polysubstance Users
Nicotine co-use is common and exacerbates sleep and mood symptoms. Concurrent nicotine withdrawal complicates attribution of symptoms. Integrated tobacco treatment can prevent substituting one driver of insomnia for another.
For individuals using alcohol or benzodiazepines, careful assessment and management of potentially dangerous withdrawal syndromes is essential.
People with Psychiatric Comorbidity
Mood disorders, anxiety disorders, and PTSD increase withdrawal severity and may delay improvement. Coordination with mental health services, extended psychosocial support, and cautious pharmacotherapy where indicated are important for this group.
What to Expect: A Realistic Prognosis
For most heavy daily cannabis users, the practical detox horizon is approximately 2 to 3 weeks for the majority of daytime symptoms, with sleep normalization extending to 4 to 6 weeks.
This timeline aligns closely with the neurobiological recovery of CB1 receptors and objective sleep architecture normalization.
Concentrate users and those with psychiatric comorbidities may need extended sleep support through day 45 or beyond.
Proactive sleep-focused behavioral care starting in the first few days of cessation, coupled with relapse prevention strategies aligned to expected peak symptom windows, provides the best balance of efficacy and safety.
With structured support, most people achieve major symptom relief and can return to normal functioning within a month.
The key is to anticipate the timeline, address sleep aggressively, integrate psychosocial therapy, and remain patient as your brain heals.
Conclusion
Marijuana withdrawal is a real, well-documented syndrome that affects nearly half of regular users who try to quit. Symptoms begin within 24 to 48 hours, peak around days 2 to 6, and largely resolve within 2 to 3 weeks, though sleep disturbances often persist for 4 to 6 weeks.
Understanding this timeline, recognizing the symptoms, and using evidence-based strategies like behavioral sleep interventions and psychosocial therapy can make the detox process more manageable and increase your chances of long-term success.
If you or someone you care about is struggling with marijuana withdrawal, professional support can make all the difference.
Thoroughbred Wellness & Recovery offers compassionate, evidence-based care tailored to your unique needs. Reach out today to explore our detox programs and take the first step toward lasting freedom.








