Why Attorneys Don’t Seek Addiction Help? Key Barriers
Georgia attorneys face elevated rates of alcohol misuse and mental health distress, yet many avoid treatment even when confidential support exists.
About 21% of practicing attorneys qualify as problem drinkers, and only 6.8% report attending treatment for substance use disorders.
The gap between need and care is not caused by lack of services. Instead, three intertwined barriers, stigma, confidentiality fears, and career concerns, stop many Georgia lawyers from seeking rehab or addiction support.
This article explains how these obstacles operate in Georgia’s legal culture and why the State Bar’s assistance infrastructure, while meaningful, has not yet fully neutralized the perceived professional risks of asking for help.
Why Georgia Attorneys Struggle with Substance Use?
Legal practice is stressful, adversarial, and demanding. National research involving 12,825 licensed attorneys found that 20.6% screened positive for hazardous drinking, while 28% experienced depression, 19% reported anxiety, and 23% faced significant stress.
These rates exceed those of other professional populations, showing that behavioral health concerns in law are common and consequential.
Georgia’s State Bar recognizes the problem. The Bar’s mental wellbeing pages explicitly address depression, stress, alcohol and drug abuse, family problems, anxiety, and burnout as lawyer wellbeing concerns requiring immediate, confidential help.
The Bar also links members to addiction resources and the ABA study on substance use, signaling institutional awareness that addiction is not rare or exceptional in the profession.
Yet awareness alone does not produce treatment. If lawyers know help exists but still avoid it, the real question is not whether services are available. The question is why using them feels unsafe.
Stigma: The Cultural Barrier Beneath Everything Else
Legal Culture Rewards Invulnerability
The most important insight from research on lawyer wellbeing is that stigma in law is structural, not merely personal. Legal workplaces often reward a robust persona. Lawyers may feel obliged to appear resilient, composed, and unaffected even when struggling.
In that environment, disclosing symptoms can feel counterintuitive because lawyers believe doing so will be seen as professional weakness.
Suppressing distress avoids immediate exposure but worsens wellbeing, functioning, and physical health. This dynamic is especially relevant to addiction support.
Rehab and substance use treatment usually require acknowledging loss of control, dependence, or dangerous coping patterns. In a profession that valorizes control, competence, stamina, and skepticism, that acknowledgment can feel identity threatening.
Psychological Dishonesty and Delayed Help Seeking
Stigma creates what researchers call “psychological dishonesty”—the gap between what lawyers experience and what they feel permitted to reveal. This concept helps explain why help seeking may be delayed even when confidential services exist.
The issue is not simply whether a lawyer technically can call a hotline. It is whether the lawyer can psychologically cross the threshold of self disclosure in a profession that often equates distress with diminished professional standing.
If a Georgia attorney believes that admitting a substance problem means admitting they are not dependable, not in command, or not safe to trust with clients, they may continue functioning in concealment until consequences force intervention.
Addiction Stigma May Be Stronger Than Mental Health Stigma
Addiction carries distinctive stigma. It is often viewed through a moralizing lens, as evidence of bad choices or weak will, rather than a treatable disorder.
Within the legal profession, addiction may be especially stigmatizing because it is easily linked in people’s minds to missed deadlines, impaired judgment, client neglect, dishonesty, or trust account mishandling.
Thus, a lawyer who might privately acknowledge anxiety may be far more reluctant to disclose alcohol or drug misuse.
Georgia’s Peer Support Design Implicitly Recognizes Stigma
Georgia’s “Lawyers Helping Lawyers” program is described as a confidential peer to peer program connecting struggling lawyers with fellow Bar members who can listen and support them around stress, depression, addiction, and other personal issues.
Peer support is not just a supplemental wellness feature. It is a strategic anti stigma intervention. It acknowledges that some lawyers may resist formal treatment initially but may be willing to talk to another lawyer who understands legal culture and can reduce the shame associated with first disclosure.
The 2024 Georgia Lawyers Helping Lawyers policies describe the LAP as including education, intervention, peer support, treatment referrals, counseling, and work/life help, showing that Georgia has intentionally built a broad assistance ecosystem rather than a narrow crisis only hotline.
Confidentiality Fears: Why “Confidential” Must Be Repeated So Often?
Georgia’s LAP Centers Confidentiality in Public Messaging
Few points are better documented in Georgia materials than the repeated emphasis on confidentiality. The State Bar’s LAP pages prominently instruct users: “Do you need immediate, confidential help? Call 800-327-9631.” State Bar promotional materials likewise describe the LAP as “a confidential service” and repeat the confidential LAP hotline.
The 2016 and 2024 Georgia Lawyers Helping Lawyers policy documents both state that the LAP is a confidential service provided by the State Bar and that, to help meet members’ needs and ensure confidentiality, the Bar contracts with an outside counseling agency.
This repeated language is significant. Institutions do not usually foreground confidentiality so aggressively unless they know confidentiality is a major obstacle to use.
Third Party Administration is Designed to Reduce Fear of Bar Exposure
Georgia’s LAP currently operates through SupportLinc/CuraLinc Healthcare. Services are routed through an external provider rather than directly through Bar disciplinary personnel. That structure matters because lawyers may fear that contacting a bar sponsored service could put them “on the radar” of regulators or employers.
By outsourcing intake and counseling, the Bar appears to be intentionally creating psychological distance between help seeking and discipline.
Why Lawyers May Still Worry, Even with Confidentiality Assurances
Even robust confidentiality messaging may not eliminate fear for several reasons:
- Lawyers think in risk terms. Attorneys are trained to ask what happens if confidentiality fails, who can access records, and what exceptions exist.
- The Bar is still the sponsor. Even where a third party administers services, some lawyers may distrust the separation or worry that serious admissions could somehow reach licensing or disciplinary channels.
- Substance use carries discovery anxiety. Lawyers may fear that treatment records, rehab participation, or admissions of addiction could surface in litigation, malpractice disputes, employment conflicts, partnership issues, or disciplinary matters.
- Professional gossip and reputation spread informally. In tight legal communities, the fear is often not only formal disclosure but informal reputational leakage.
- Confidentiality and anonymity are not the same. A lawyer may understand that a program is “confidential” in a formal sense but still feel personally exposed by using it.
Georgia’s Structure Suggests Policymakers Know This Fear is Real
The current LAP offers multiple access points, hotline, email, web portal, digital modalities, real time scheduling, text therapy, anonymous virtual group support, and peer assistance.
These options lower the threshold for first contact and allow a lawyer to seek help in ways that may feel less visible than walking into a clinic or disclosing to an employer.
The 2020 Georgia flyer states that there is no cost to use the program, that all sessions are strictly confidential, and that members receive six clinical sessions per year with an independent licensed counselor near their office or home.
The same flyer references confidentiality under Part VII, Lawyer Assistance Program, Rule 7-303, further signaling that formal rule based confidentiality protections exist or are at least publicly invoked in LAP messaging.
Career Concerns: Why Help Seeking Can Feel Professionally Dangerous?
Addiction is Easily Associated with Professional Impairment
Georgia’s LAP materials explicitly state that the program is meant to help members with problems that negatively affect both quality of life and their ability to function effectively as lawyers.
This framing is humane and functional rather than punitive, but it also reveals why lawyers may fear seeking treatment: substance problems can be read as threats to practice capacity.
The Georgia Rules of Professional Conduct govern competence, diligence, communication, fees, confidentiality, and other core duties.
A lawyer struggling with addiction may reasonably worry that admitting the problem could invite questions about whether they have already failed clients, missed deadlines, mishandled funds, or otherwise violated professional duties.
Georgia Disciplinary Processes Can Intensify Perceived Risk
The Bar’s disciplinary process page states that the early stages of an investigation are completely confidential, with public discipline appearing only after action by the Supreme Court of Georgia. That confidentiality is protective.
However, the same page also states that under Bar Rule 4-104, the State Disciplinary Board may refer a lawyer for a medical or mental health evaluation if there are signs of mental illness, cognitive impairment, alcohol abuse, or substance abuse, and that the referral is confidential.
This is a nuanced point. Formally, the Bar is saying early investigations and evaluation referrals are confidential. But psychologically, a lawyer may hear something different: substance issues can trigger regulatory attention.
Even if the process is confidential, the prospect of being evaluated for impairment within a disciplinary framework may reinforce the belief that addiction is professionally dangerous to disclose.
Fear of Being Seen as Weak, Unreliable, or Unfit
Stigma in legal workplaces makes lawyers fear appearing weak or professionally compromised, and workplace cultures often reward a façade of toughness and invulnerability. In practical terms, that can translate into multiple career anxieties:
- Partners may stop staffing the lawyer on important matters
- Clients may lose confidence
- Colleagues may see the lawyer as unstable or unsafe
- Judges or opposing counsel may treat the lawyer differently
- Advancement opportunities may narrow
- Lateral moves may become harder
- Recovery may not erase the reputational label
These concerns are not explicitly catalogued in Georgia’s official pages, but they are strongly supported by the literature on legal culture and are entirely consistent with why Georgia’s assistance program foregrounds confidentiality and peer support.
How Stigma, Confidentiality Fear, and Career Concerns Interact?
These barriers should not be treated as separate boxes. They reinforce each other.
Stigma drives confidentiality fear: If addiction were viewed simply as a treatable health condition, confidentiality would matter but would not dominate the analysis. Confidentiality becomes critical because disclosure is stigmatized. Lawyers seek secrecy not merely for privacy’s sake but because they expect reputational or professional penalties if others know.
Confidentiality fear magnifies career concern: When lawyers are unsure who might learn of treatment, they imagine worst case career outcomes. This is especially true in legal practice, where uncertainty itself can deter action. Even if the actual probability of disclosure is low, perceived uncertainty can be enough to stop help seeking.
Career concern deepens stigma: The more lawyers believe that addiction marks them as unfit, unreliable, or weak, the more the stigma becomes internalized. At that point, the barrier is not only “what others will think” but “what admitting this says about me as a lawyer.”
Georgia’s Support Infrastructure: Stronger Than Minimal, But Not Strong Enough to Defeat Culture Alone
Georgia Has Built a Broad Support System
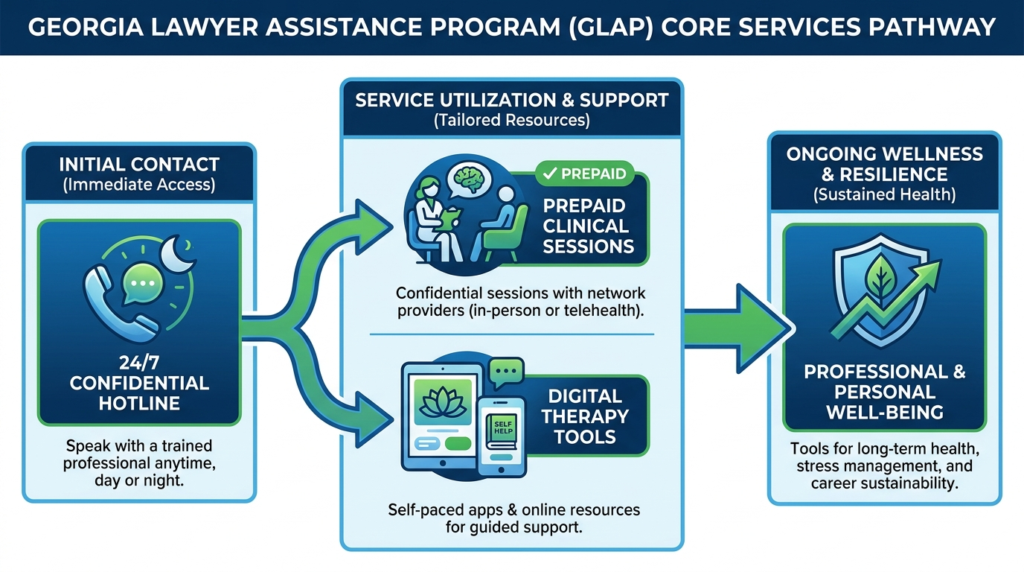
A key finding from the deeper Georgia materials is that the State Bar has not limited itself to a bare hotline. The 2024 Lawyers Helping Lawyers policies describe a broad network including:
- A 24/7 confidential hotline
- Up to six prepaid in person counseling sessions per year
- Peer support
- Education
- Intervention
- Clinical treatment referrals
- Unlimited work/life assistance for issues such as child care, elder care, and finances
The current State Bar webpage adds digital features such as real time scheduling, a mental health navigator, text therapy, digital cognitive behavioral therapy, anonymous virtual group support, and web based access through SupportLinc.
This is a substantial infrastructure by bar association standards.

Cost Barriers Have Been Partially Reduced
The Bar emphasizes that members are entitled to six prepaid clinical sessions per calendar year. The 2020 flyer states there is no cost for a State Bar member to use the program for those sessions.
Reducing cost does not remove all treatment barriers, especially for longer term rehab, but it lowers the threshold for early intervention.
Still, Support Availability Does Not Equal Trust
The existence of a robust infrastructure does not by itself prove that it fully overcomes help seeking barriers. In fact, one can read the breadth of the program as evidence of how high the barriers are.
If lawyers needed only a phone number, there would be less need for third party administration, peer support, text therapy, anonymous group sessions, and repeated confidentiality messaging.
Why Peer Support Matters So Much in Georgia?
Georgia’s Lawyers Helping Lawyers program offers a fellow Bar member “to be there, listen and help.” This is not trivial. Peer support can reduce all three barriers at once:
- Stigma: “another lawyer has been through this” normalizes distress
- Confidentiality fear: a first conversation may feel less formal than therapy or rehab intake
- Career concern: a peer can model survival, recovery, and continued professionalism
Substance use disorders often involve shame, denial, and ambivalence. A lawyer may reject the idea of “rehab” but accept a confidential conversation with another lawyer in recovery or with lived knowledge of the profession’s pressures. Thus peer support can function as the least threatening gateway into formal treatment.
The Lawyers Who Most Need Rehab May Be the Least Likely to Seek It Voluntarily
This is the hardest truth in the research. Earlier stage stress or anxiety may be easier to bring to a confidential peer or counselor. But once substance use threatens actual performance, the lawyer’s fear of career consequences intensifies, making voluntary treatment less likely right when it is most necessary.
A likely sequence for some Georgia attorneys is:
1. Stress, trauma, burnout, or professional pressure intensifies
2. Alcohol or drugs become coping tools
3. The lawyer recognizes the problem privately
4. Stigma makes disclosure feel like weakness
5. Confidentiality worries make help seem unsafe
6. Career concerns make treatment feel potentially more dangerous than concealment
7. Symptoms worsen, functioning declines, and risk increases
This sequence is strongly consistent with research describing symptom suppression and the profession’s façade of invulnerability.
What the Evidence Suggests About Different Attorney Subgroups?
Younger Lawyers
National research found younger attorneys and those earlier in practice were more likely to have higher alcohol use scores. Younger Georgia lawyers may therefore face a concerning combination: elevated risk, lower professional security, stronger admissions/credentialing anxiety, and fear of being permanently labeled early in career.
Lawyers in High Stress Practice Areas
Georgia lawyers in criminal defense, family law, personal injury, child advocacy, and other trauma exposed practices may be especially vulnerable to self medication, while also feeling pressure to project toughness.
Solo and Small Firm Lawyers
Solo and small firm practitioners likely face heightened confidentiality and career concerns because there is no internal HR or protected leave structure, reputation in local networks is crucial, any absence for rehab may be harder to conceal, and client service disruption is immediate.
Judges and Quasi Judicial Roles
Georgia’s current LAP page states that if you are a lawyer or judge with a personal problem causing significant concern, the confidential hotline can help. For judges, the stakes may be even higher because authority and public legitimacy are central to the role, likely magnifying stigma and confidentiality fears.
Objective Evaluation of the Strongest Explanations
Based on the supplied evidence, several explanations for treatment avoidance are plausible. The question is which are strongest.
Weak explanation: Georgia lacks support resources. This explanation is not supported. Georgia has a meaningful assistance infrastructure, including confidential hotline access, counseling, peer support, treatment referral, digital tools, and work/life help.
Moderate explanation: Cost alone stops attorneys. Cost likely matters, but Georgia’s prepaid session model reduces early cost barriers. Cost is not the main story, particularly relative to stigma and career fear.
Strong explanation: Legal culture stigmatizes vulnerability. This is strongly supported by the deeper literature, especially research on trauma informed legal practice.
Strong explanation: Lawyers fear confidentiality breaches or formal exposure. This is strongly supported indirectly by Georgia’s repeated confidentiality branding and use of third party providers, plus the general logic of lawyer help seeking in a regulated profession.
Strong explanation: Lawyers fear career damage if addiction becomes known. This is strongly supported by the interaction between legal culture stigma, professional duties, and Georgia’s discipline framework.
The Bottom Line
Georgia attorneys practice within a profession known for high stress, meaningful rates of problematic drinking, and substantial mental health burden.
The State Bar of Georgia has responded with a relatively robust support structure: confidential hotlines, third party counseling administration, six prepaid sessions, peer assistance, treatment referrals, work/life support, and digital access. Those features matter and likely help many lawyers.
But the strongest conclusion from the integrated evidence is that the central obstacle is not service scarcity, it is professional risk perception.
Stigma tells lawyers that needing rehab signals weakness. Confidentiality fears make them question whether getting help can remain private. Career concerns make treatment feel potentially dangerous to reputation, client confidence, and licensure.
Georgia’s disciplinary framework, while partly confidential and not inherently punitive in all cases, still reinforces the idea that substance related impairment can have regulatory consequences.
The result is a predictable pattern: lawyers may hide distress, self manage too long, delay formal treatment, and seek help only when the problem has worsened.
Thus, the answer to the query is not that Georgia lawyers fail to seek addiction support because they are indifferent or uninformed. They often avoid it because, in the legal profession’s current culture, admitting the problem can feel riskier than continuing it in secret.
If you or someone you know is a Georgia attorney struggling with substance use, confidential help is available right here. Thoroughbred Wellness & Recovery offers dual diagnosis treatment designed for professionals who need compassionate, evidence based care without judgment. Call us today to speak with our specialist!