Lamictal and Zoloft: Can You Take Zoloft & Lamictal Together?
Many people wonder whether they can safely combine Lamictal and Zoloft, especially when managing both mood disorders and anxiety or depression. The short answer is yes! These medications can often be taken together under medical supervision.
A 2012 retrospective study found no statistically significant interaction between the two drugs in psychiatric patients, though the study was small and could not rule out individual variation. This article will explain what the research shows, what risks to watch for, and how to use these medications safely together.
Understanding Lamictal and Zoloft
Lamictal, the brand name for lamotrigine, is an anticonvulsant and mood stabilizer approved for epilepsy and maintenance treatment of bipolar I disorder.
According to current prescribing information, it works primarily to delay mood episodes in patients already treated for acute symptoms.
Recent clinical practice guidelines emphasize that lamotrigine is most effective for preventing depressive episodes rather than manic ones, and it must be started slowly to reduce the risk of serious rash.
Zoloft, or sertraline, is a selective serotonin reuptake inhibitor commonly prescribed for major depression, anxiety disorders, panic disorder, obsessive-compulsive disorder, and post-traumatic stress disorder. It works by increasing serotonin levels in the brain, which helps regulate mood and anxiety.
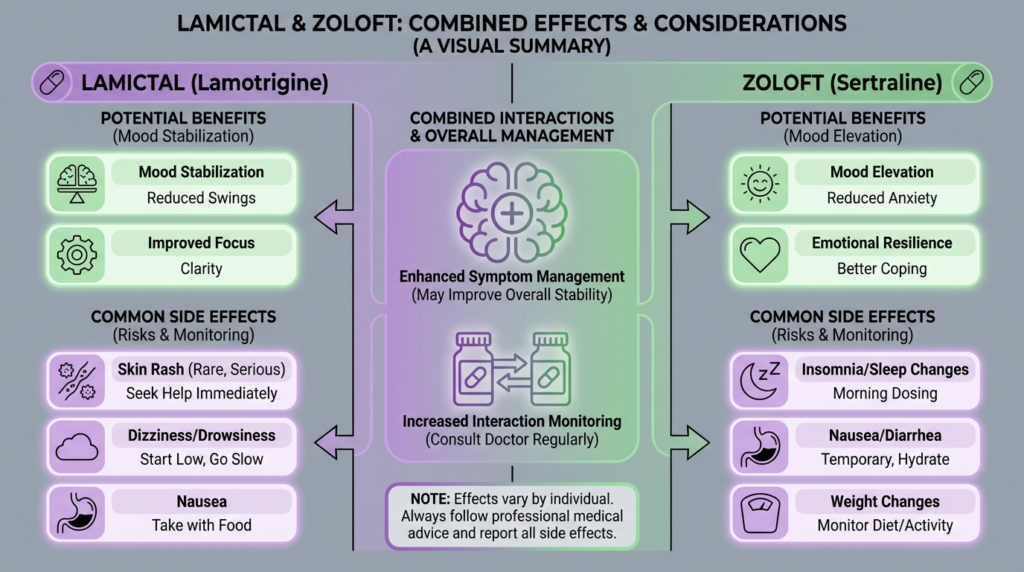
The two medications address different but overlapping problems. Lamictal provides long-term mood stabilization and helps prevent depressive relapses in bipolar disorder. Zoloft targets acute depressive symptoms, anxiety, panic, and obsessive thoughts.
This complementary action explains why doctors often prescribe them together, particularly for patients with bipolar disorder who also experience significant anxiety or persistent depression.
What the Research Shows About Taking Them Together?
The Evidence is Mixed but Generally Reassuring
The interaction between Zoloft and Lamictal has been studied directly, though the evidence base remains limited. The most important research includes a concerning early case report and a later, more reassuring observational study.
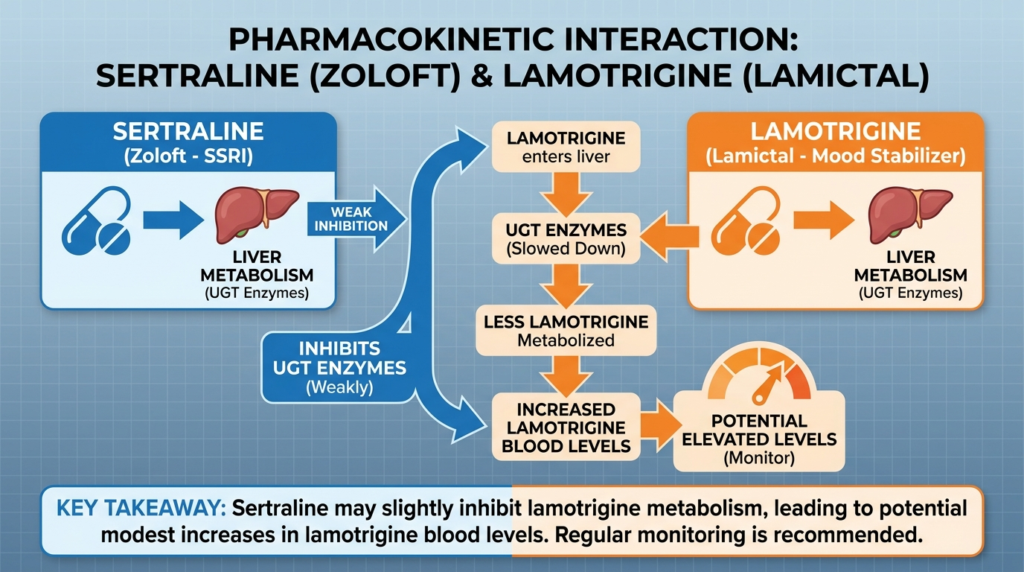
In 1998, researchers published a case report describing two epilepsy patients who experienced marked changes in lamotrigine blood levels after starting or stopping sertraline.
In one case, adding just 25 mg daily of sertraline appeared to double the lamotrigine level and cause toxicity symptoms. The authors suggested that sertraline might inhibit lamotrigine metabolism and recommended careful monitoring.
However, a 2012 retrospective study painted a different picture. Researchers compared lamotrigine blood levels in psychiatric patients taking sertraline versus those not taking it. They found dose-corrected lamotrigine concentrations of 60.4 versus 51.1 μmol/L × 1,000/mg/day, a difference that was not statistically significant with a p-value of 0.42.
The authors concluded that any effect of sertraline on lamotrigine metabolism was not clinically significant, though they acknowledged their small sample size of only seven patients taking both drugs meant they could have missed a real effect.
A 2024 review of pharmacokinetic interactions between antiseizure and psychiatric medications summarized the tension in the evidence: early cases suggested a possible interaction, but later analysis found only a slight, non-significant increase in lamotrigine levels.
What This Means for You?
The best interpretation of the available evidence is that most people can take Zoloft and Lamictal together without major problems, but the combination is not entirely interaction-free.
A large, consistent pharmacokinetic interaction has not been proven, but individual patients may experience meaningful changes in lamotrigine levels when sertraline is started, stopped, or adjusted.
Current lamotrigine prescribing information does not list sertraline among the major drug interactions that require automatic dose adjustments, unlike valproate, carbamazepine, or estrogen-containing contraceptives.
This regulatory silence suggests the interaction is not considered a major clinical concern at the population level.
Potential Benefits of the Combination
Complementary Symptom Relief
The primary benefit of combining Lamictal and Zoloft is that they target different aspects of mood and anxiety disorders.
Lamictal excels at long-term mood stabilization and preventing depressive relapses in bipolar disorder, while Zoloft addresses acute symptoms like persistent sadness, worry, panic attacks, and obsessive thoughts.
For someone with bipolar disorder who remains anxious or mildly depressed despite mood stabilization, adding Zoloft may provide additional relief.
Similarly, a patient initially treated for depression and anxiety with Zoloft who later shows signs of bipolar spectrum illness may benefit from adding Lamictal for mood stability.
Supported by Bipolar Treatment Guidelines
Recent bipolar disorder guidelines note that adjunctive antidepressant treatment may be considered as a second-line option for acute bipolar depression.
The guidelines specifically state that SSRIs like Zoloft or bupropion are preferred because they have lower rates of triggering manic episodes compared with other antidepressants.
However, the guidelines emphasize that antidepressants should never be used alone in bipolar disorder and must be combined with an adequate mood stabilizer like Lamictal.
This evidence-based framework supports the Lamictal-Zoloft combination when there is a clear clinical need, proper monitoring, and patient education about warning signs of mood destabilization.
Better Tolerability Than Some Alternatives
Compared with some other mood stabilizers and antipsychotics, Lamictal tends to have a more favorable side effect profile.
It typically does not cause significant weight gain or metabolic problems, and many patients find it less sedating than alternatives. Zoloft is similarly well-tolerated by many people and offers flexible dosing options.
When both medications work well together, patients may achieve better symptom control with fewer troublesome side effects than they might experience with higher doses of a single medication or with different drug combinations.
Important Risks and Side Effects
Serious Rash Risk from Lamictal
The most important safety concern when taking Lamictal is the risk of serious skin reactions, including Stevens-Johnson syndrome and toxic epidermal necrolysis. These potentially life-threatening rashes are more likely when Lamictal is started too quickly, at too high a dose, or when combined with valproate.
According to official safety information, nearly all serious rashes occur within the first two to eight weeks of treatment. The risk increases dramatically when the recommended titration schedule is not followed. Patients should stop Lamictal immediately at the first sign of any rash unless it is clearly not drug-related.
This rash risk exists whether or not you take Zoloft. However, when starting both medications or adjusting doses, patients and doctors must remain vigilant because new symptoms could be mistakenly attributed to the “new” medication while missing an important Lamictal warning sign.
Possible Lamictal Toxicity in Some Individuals
Although the average interaction between Zoloft and Lamictal appears small, some individuals may experience increased lamotrigine levels when sertraline is added. Symptoms of lamotrigine toxicity can include dizziness, loss of balance, blurred or double vision, confusion, excessive drowsiness, and nausea.
If you develop these symptoms after starting Zoloft or increasing the dose, contact your doctor promptly. They may check your lamotrigine blood level and adjust your dose if needed.
Additive Central Nervous System Effects
Even without a major pharmacokinetic interaction, taking two psychiatric medications together can increase side effects like drowsiness, dizziness, cognitive slowing, and coordination problems. These effects may be most noticeable during the first few weeks of treatment or after dose changes.
Alcohol can worsen these effects significantly, so it is important to discuss alcohol use with your doctor and follow their recommendations about limiting or avoiding it while taking these medications.
Risk of Mood Switching in Bipolar Disorder
One of the most important risks specific to bipolar disorder is that antidepressants like Zoloft can sometimes trigger a switch into hypomania or mania.
Current guidelines emphasize that antidepressants should be used cautiously in bipolar disorder, always with a mood stabilizer, and discontinued promptly if a treatment-emergent mood switch occurs.
Warning signs of a possible switch include decreased need for sleep, racing thoughts, increased energy that feels “revved up” rather than healthy, impulsive spending or risk-taking, irritability, pressured speech, and grandiose thinking.
Special Considerations for Older Adults
Prescribing information notes that older adults should start Lamictal at lower doses and increase more slowly because of greater risk of liver, kidney, or heart problems and increased sensitivity to side effects.
Older adults taking Zoloft are also at higher risk for hyponatremia, a dangerous drop in sodium levels that can cause confusion, lethargy, and falls.
What to Monitor When Taking Both Medications?
Watch for These Symptoms
When taking Lamictal and Zoloft together, pay close attention to:
- Any new rash, especially in the first eight weeks of Lamictal treatment
- Dizziness, loss of balance, or coordination problems
- Blurred vision or double vision
- Unusual drowsiness or confusion
- Nausea or vomiting
- Decreased need for sleep or racing thoughts (possible mood switch)
- Worsening anxiety in the first one to two weeks (common early Zoloft effect that usually improves)
- Changes in seizure frequency if you take Lamictal for epilepsy
When to Contact Your Doctor Immediately
Seek medical attention right away if you develop:
- Any rash, blistering, or peeling skin
- Painful sores in your mouth or around your eyes
- Fever with rash
- Severe dizziness or inability to walk steadily
- Marked confusion or disorientation
- Signs of a manic episode such as greatly decreased sleep, reckless behavior, or racing thoughts
Laboratory Monitoring
Routine blood level monitoring of lamotrigine is not standard practice for most patients. However, your doctor may order a lamotrigine level if you develop symptoms suggesting toxicity, if your seizures or mood symptoms worsen unexpectedly, or if there are concerns about medication adherence.
If you are older or develop unexplained lethargy or confusion while taking Zoloft, your doctor may check your sodium level to rule out hyponatremia.
Proper Dosing and Titration
Lamictal Must Be Started Slowly
The single most important safety measure when taking Lamictal is following the recommended titration schedule. Clinical guidelines emphasize that rapid titration is a frequent cause of serious rash and that the standard protocol must be followed carefully.
For bipolar disorder, Lamictal is typically started at a low dose and increased gradually over several weeks to a target maintenance dose around 200 mg daily, though some patients need higher or lower doses. The exact schedule depends on what other medications you take, particularly whether you are on valproate or enzyme-inducing drugs.
Zoloft Dosing Flexibility
Zoloft is often started at a low dose, such as 25 or 50 mg daily, and increased after one to two weeks if tolerated. For anxiety disorders, starting low is especially important because anxiety can temporarily worsen in the first week or two. Full benefits for anxiety or OCD may take up to three months to appear.
No Automatic Dose Adjustments Needed
Based on current evidence, you should not automatically change the dose of either medication simply because you are taking them together. Dose adjustments should be based on your clinical response, side effects, and any symptoms suggesting toxicity, not on the theoretical possibility of an interaction.
Comparing the Zoloft Interaction to Other Lamictal Interactions
It helps to put the Zoloft-Lamictal interaction in perspective by comparing it with other, better-established lamotrigine interactions.
| Interacting medication | Effect on lamotrigine levels | Clinical importance |
|---|---|---|
| Valproate | Increases levels more than 2-fold | Very high (dose adjustment required) |
| Estrogen contraceptives | Decreases levels by about 50% | Very high (dose adjustment often needed) |
| Carbamazepine, phenytoin | Decreases levels by about 40% | High (dose adjustment often needed) |
| Sertraline (Zoloft) | Small or inconsistent effect | Moderate (monitor but usually no automatic adjustment) |
This table shows that the Zoloft interaction, while worth monitoring, is not in the same category as the major, well-established lamotrigine interactions that require routine dose changes.
What to Expect When Starting Both Medications?
Weeks One to Two
During the first two weeks, Lamictal will still be at a low dose as it is titrated upward. If you are starting Zoloft at the same time, you may notice mild gastrointestinal upset, jitteriness, or temporary worsening of anxiety. These early Zoloft effects often improve within a week or two.
Headache, mild dizziness, or sleep changes may occur from either medication. Any new rash during this period requires immediate medical attention.
Weeks Three to Six
As Lamictal continues to increase and Zoloft begins to show clearer benefits, you may start to notice improvement in mood and anxiety symptoms. If the combination is going to cause notable dizziness, cognitive fog, or coordination problems, these effects often emerge during this period or after dose increases.
If you have bipolar disorder, your doctor should check carefully for any signs of activation or reduced sleep that might signal a mood switch.
Weeks Six to Twelve
By this point, Lamictal may be approaching its therapeutic maintenance dose, and Zoloft’s benefits should be more apparent. The key question becomes whether you are actually more stable and less symptomatic, not just tolerating the medications.
Long-Term Expectations
Lamictal’s greatest value often becomes visible over months as it helps prevent depressive relapses. The need for continued Zoloft should be reviewed periodically with your doctor, particularly in bipolar disorder where the optimal duration of antidepressant treatment remains uncertain.
When the Combination May Not Be Right?
While Lamictal and Zoloft can often be used together safely, the combination may not be appropriate in certain situations:
- Bipolar disorder with predominantly manic symptoms or recent mania, where an antidepressant could worsen instability
- Rapid-cycling bipolar disorder, where antidepressants may increase cycle frequency
- History of severe antidepressant-induced mania
- Inability to follow the slow Lamictal titration schedule due to adherence concerns
- Active substance use that could interfere with medication adherence or increase risk of adverse effects
- Severe liver or kidney disease requiring more cautious dosing and monitoring
Your doctor will consider your complete medical and psychiatric history, current symptoms, other medications, and individual risk factors when deciding whether this combination is right for you.
The Bottom Line
Lamictal and Zoloft can often be taken together safely and effectively, particularly for people with bipolar disorder who need both mood stabilization and treatment for depression or anxiety.
The evidence suggests that a major, consistent drug interaction is unlikely, though individual patients may experience changes in lamotrigine levels when sertraline is started or adjusted.
The most important safety measures are following the slow Lamictal titration schedule to minimize rash risk, monitoring closely for side effects during the first weeks and after dose changes, watching for signs of mood switching in bipolar disorder, and maintaining open communication with your doctor about any new or concerning symptoms.
This combination represents a reasonable, evidence-based approach when there is a clear clinical need, but it should never be started casually or without proper medical supervision and follow-up.
If you are struggling with co-occurring mood and anxiety symptoms and wondering whether medication adjustments might help, reach out to our qualified treatment team.
At Thoroughbred Wellness & Recovery, our dual diagnosis treatment approach addresses both substance use and mental health concerns with personalized, compassionate care that includes medication management, individual therapy, and holistic support.